Damien M. Wu MD , Michael Z.L. Zhu MBBS , Edward Buratto MBBS, PhD, FRACS , Christian P. Brizard MD, MS , Igor E. Konstantinov MD, PhD, FRACS
{"title":"Aortic Valve Surgery in Children With Infective Endocarditis","authors":"Damien M. Wu MD , Michael Z.L. Zhu MBBS , Edward Buratto MBBS, PhD, FRACS , Christian P. Brizard MD, MS , Igor E. Konstantinov MD, PhD, FRACS","doi":"10.1053/j.semtcvs.2023.02.004","DOIUrl":null,"url":null,"abstract":"<div><div><span>There is limited data on the outcomes of children who undergo surgery for aortic valve<span><span> infective endocarditis (IE), and the optimal surgical approach remains controversial. We investigated the long-term outcomes of surgery for aortic valve IE in children, with a particular focus on the Ross procedure<span>. A retrospective review of all children who underwent surgery for aortic valve IE was performed at a single institution. Between 1989 and 2020, 41 children underwent surgery for aortic valve IE, of whom 16 (39.0%) underwent valve repair, 13 (31.7%) underwent the Ross procedure, 9 (21.9%) underwent a </span></span>homograft<span><span> root replacement, and 3 (7.3%) underwent a mechanical valve replacement. Median age was 10.1 years (interquartile range, 5.4–14.1). The majority of children (82.9%, 34/41) had underlying congenital heart disease, while 39.0% (16/41) had previous heart surgery. </span>Operative mortality was 0.0% (0/16) for repair, 15.4% (2/13) for the Ross procedure, 33.3% (3/9) for homograft root replacement, and 33.3% (1/3) for mechanical replacement. Survival at 10 years was 87.5% for repair, 74.1% for Ross, and 66.7% for homograft (</span></span></span><em>P</em><span> > 0.05). Freedom from reoperation at 10 years was 30.8% for repair, 63.0% for Ross, and 26.3% for homograft (</span><em>P</em> = 0.15 for Ross vs repair, <em>P</em> = 0.002 for Ross vs homograft). Children undergoing surgery for aortic valve IE have acceptable long-term survival, although the need for long-term reintervention is significant. The Ross procedure appears to be the optimal choice when repair is not feasible.</div></div>","PeriodicalId":48592,"journal":{"name":"Seminars in Thoracic and Cardiovascular Surgery","volume":"36 4","pages":"Pages 418-427"},"PeriodicalIF":2.5000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Seminars in Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1043067923000382","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
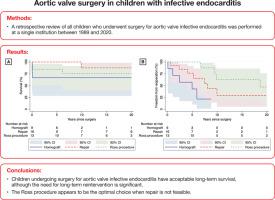
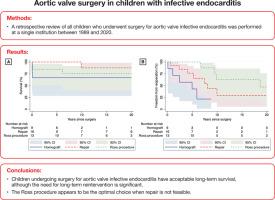
There is limited data on the outcomes of children who undergo surgery for aortic valve infective endocarditis (IE), and the optimal surgical approach remains controversial. We investigated the long-term outcomes of surgery for aortic valve IE in children, with a particular focus on the Ross procedure. A retrospective review of all children who underwent surgery for aortic valve IE was performed at a single institution. Between 1989 and 2020, 41 children underwent surgery for aortic valve IE, of whom 16 (39.0%) underwent valve repair, 13 (31.7%) underwent the Ross procedure, 9 (21.9%) underwent a homograft root replacement, and 3 (7.3%) underwent a mechanical valve replacement. Median age was 10.1 years (interquartile range, 5.4–14.1). The majority of children (82.9%, 34/41) had underlying congenital heart disease, while 39.0% (16/41) had previous heart surgery. Operative mortality was 0.0% (0/16) for repair, 15.4% (2/13) for the Ross procedure, 33.3% (3/9) for homograft root replacement, and 33.3% (1/3) for mechanical replacement. Survival at 10 years was 87.5% for repair, 74.1% for Ross, and 66.7% for homograft (P > 0.05). Freedom from reoperation at 10 years was 30.8% for repair, 63.0% for Ross, and 26.3% for homograft (P = 0.15 for Ross vs repair, P = 0.002 for Ross vs homograft). Children undergoing surgery for aortic valve IE have acceptable long-term survival, although the need for long-term reintervention is significant. The Ross procedure appears to be the optimal choice when repair is not feasible.
期刊介绍:
Seminars in Thoracic and Cardiovascular Surgery is devoted to providing a forum for cardiothoracic surgeons to disseminate and discuss important new information and to gain insight into unresolved areas of question in the specialty. Each issue presents readers with a selection of original peer-reviewed articles accompanied by editorial commentary from specialists in the field. In addition, readers are offered valuable invited articles: State of Views editorials and Current Readings highlighting the latest contributions on central or controversial issues. Another prized feature is expert roundtable discussions in which experts debate critical questions for cardiothoracic treatment and care. Seminars is an invitation-only publication that receives original submissions transferred ONLY from its sister publication, The Journal of Thoracic and Cardiovascular Surgery. As we continue to expand the reach of the Journal, we will explore the possibility of accepting unsolicited manuscripts in the future.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
