Maciej Stąpór , Dorota Sobczyk , Grzegorz Wasilewski , Karol Wierzbicki , Andrzej Gackowski , Paweł Kleczyński , Krzysztof Żmudka , Bogusław Kapelak , Jacek Legutko
{"title":"Right ventricular–pulmonary arterial coupling in patients with implanted left ventricular assist devices","authors":"Maciej Stąpór , Dorota Sobczyk , Grzegorz Wasilewski , Karol Wierzbicki , Andrzej Gackowski , Paweł Kleczyński , Krzysztof Żmudka , Bogusław Kapelak , Jacek Legutko","doi":"10.1016/j.hjc.2023.06.002","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><p>Both the right ventricular (RV) contractile function and pulmonary arterial (PA) pressure influence clinical outcomes in patients supported with left ventricular assist devices (LVADs), but the impact of RV-PA coupling is unknown. This study aimed to determine the prognostic impact of RV-PA coupling in patients with implanted LVADs.</p></div><div><h3>Methods</h3><p>Patients with implanted third-generation LVADs were retrospectively enrolled. The RV-PA coupling was assessed preoperatively by the ratio of RV free wall strain (RVFWS) derived from speckle-tracking echocardiography and noninvasively measured peak RV systolic pressure (RVSP). The primary end point was a composite of all-cause mortality or right heart failure (RHF) hospitalization. Secondary end points consisted of all-cause mortality at a 12-month follow-up and RHF hospitalization.</p></div><div><h3>Results</h3><p>A total of 103 patients were screened, and 72 with good RV myocardial imaging were included. The median age was 57 years; 67 patients (93.1%) were men, and 41 (56,9%) had dilated cardiomyopathy. A receiver-operating characteristic analysis (AUC 0.703, 51.5% sensitivity, 94.9% specificity) was used to identify the optimal cutoff point (0.28%/mmHg) for the RVFWS/TAPSE threshold. Nineteen subjects (26.4%) had advanced RV-PA uncoupling. Event rates were estimated using the Kaplan-Meier method showing a strong association with an increased risk for the primary end point of death or RHF hospitalization (89.47% vs. 30.19%, p < 0.001). A similar observation applied to all-cause mortality (47.37% vs. 13.21%, p = 0.003) and RHF hospitalization (80.43% vs. 20%, p < 0.001).</p></div><div><h3>Conclusions</h3><p>An advanced RV dysfunction assessed by RV-PA coupling may serve as a predictor of adverse outcomes in patients with implanted LVADs.</p></div>","PeriodicalId":55062,"journal":{"name":"Hellenic Journal of Cardiology","volume":"77 ","pages":"Pages 44-53"},"PeriodicalIF":3.0000,"publicationDate":"2024-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S1109966623001070/pdfft?md5=2d3fc1eca500f9140cbe70c35fb945fb&pid=1-s2.0-S1109966623001070-main.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hellenic Journal of Cardiology","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1109966623001070","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Objective
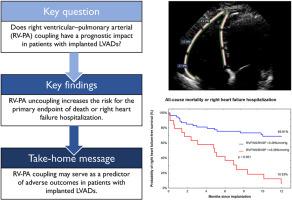
Both the right ventricular (RV) contractile function and pulmonary arterial (PA) pressure influence clinical outcomes in patients supported with left ventricular assist devices (LVADs), but the impact of RV-PA coupling is unknown. This study aimed to determine the prognostic impact of RV-PA coupling in patients with implanted LVADs.
Methods
Patients with implanted third-generation LVADs were retrospectively enrolled. The RV-PA coupling was assessed preoperatively by the ratio of RV free wall strain (RVFWS) derived from speckle-tracking echocardiography and noninvasively measured peak RV systolic pressure (RVSP). The primary end point was a composite of all-cause mortality or right heart failure (RHF) hospitalization. Secondary end points consisted of all-cause mortality at a 12-month follow-up and RHF hospitalization.
Results
A total of 103 patients were screened, and 72 with good RV myocardial imaging were included. The median age was 57 years; 67 patients (93.1%) were men, and 41 (56,9%) had dilated cardiomyopathy. A receiver-operating characteristic analysis (AUC 0.703, 51.5% sensitivity, 94.9% specificity) was used to identify the optimal cutoff point (0.28%/mmHg) for the RVFWS/TAPSE threshold. Nineteen subjects (26.4%) had advanced RV-PA uncoupling. Event rates were estimated using the Kaplan-Meier method showing a strong association with an increased risk for the primary end point of death or RHF hospitalization (89.47% vs. 30.19%, p < 0.001). A similar observation applied to all-cause mortality (47.37% vs. 13.21%, p = 0.003) and RHF hospitalization (80.43% vs. 20%, p < 0.001).
Conclusions
An advanced RV dysfunction assessed by RV-PA coupling may serve as a predictor of adverse outcomes in patients with implanted LVADs.
目的:右心室(RV)收缩功能和肺动脉(PA)压力都影响左心室辅助装置(lvad)患者的临床结果,但RV-PA耦合的影响尚不清楚。本研究旨在确定RV-PA偶联对植入lvad患者预后的影响。方法:对植入第三代lvad的患者进行回顾性研究。术前通过斑点跟踪超声心动图得出的左室游离壁应变(RVFWS)与无创测量的左室收缩压峰值(RVSP)之比评估左室- pa耦合。主要终点是全因死亡率或右心衰(RHF)住院率的综合。次要终点包括随访12个月的全因死亡率和RHF住院。结果:共筛选103例患者,纳入72例右室心肌显像良好的患者。中位年龄为57岁;67例(93.1%)为男性,41例(56.9%)为扩张型心肌病。采用受体工作特征分析(AUC为0.703,灵敏度为51.5%,特异性为94.9%)确定RVFWS/TAPSE阈值的最佳截断点(0.28%/mmHg)。19例(26.4%)患者有晚期RV-PA解耦。使用Kaplan-Meier方法估计事件发生率,结果显示与主要终点死亡或RHF住院的风险增加密切相关(89.47% vs. 30.19%)。结论:通过RV- pa耦合评估的晚期RV功能障碍可作为植入lvad患者不良结局的预测因子。
期刊介绍:
The Hellenic Journal of Cardiology (International Edition, ISSN 1109-9666) is the official journal of the Hellenic Society of Cardiology and aims to publish high-quality articles on all aspects of cardiovascular medicine. A primary goal is to publish in each issue a number of original articles related to clinical and basic research. Many of these will be accompanied by invited editorial comments.
Hot topics, such as molecular cardiology, and innovative cardiac imaging and electrophysiological mapping techniques, will appear frequently in the journal in the form of invited expert articles or special reports. The Editorial Committee also attaches great importance to subjects related to continuing medical education, the implementation of guidelines and cost effectiveness in cardiology.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
