Cristobal Rodero, Tiffany M G Baptiste, Rosie K Barrows, Hamed Keramati, Charles P Sillett, Marina Strocchi, Pablo Lamata, Steven A Niederer
{"title":"A systematic review of cardiac <i>in-silico</i> clinical trials.","authors":"Cristobal Rodero, Tiffany M G Baptiste, Rosie K Barrows, Hamed Keramati, Charles P Sillett, Marina Strocchi, Pablo Lamata, Steven A Niederer","doi":"10.1088/2516-1091/acdc71","DOIUrl":null,"url":null,"abstract":"<p><p>Computational models of the heart are now being used to assess the effectiveness and feasibility of interventions through <i>in-silico</i> clinical trials (ISCTs). As the adoption and acceptance of ISCTs increases, best practices for reporting the methodology and analysing the results will emerge. Focusing in the area of cardiology, we aim to evaluate the types of ISCTs, their analysis methods and their reporting standards. To this end, we conducted a systematic review of cardiac ISCTs over the period of 1 January 2012-1 January 2022, following the preferred reporting items for systematic reviews and meta-analysis (PRISMA). We considered cardiac ISCTs of human patient cohorts, and excluded studies of single individuals and those in which models were used to guide a procedure without comparing against a control group. We identified 36 publications that described cardiac ISCTs, with most of the studies coming from the US and the UK. In <math><mn>75</mn><mi>%</mi></math> of the studies, a validation step was performed, although the specific type of validation varied between the studies. ANSYS FLUENT was the most commonly used software in <math><mn>19</mn><mi>%</mi></math> of ISCTs. The specific software used was not reported in <math><mn>14</mn><mi>%</mi></math> of the studies. Unlike clinical trials, we found a lack of consistent reporting of patient demographics, with <math><mn>28</mn><mi>%</mi></math> of the studies not reporting them. Uncertainty quantification was limited, with sensitivity analysis performed in only <math><mn>19</mn><mi>%</mi></math> of the studies. In <math><mn>97</mn><mi>%</mi></math> of the ISCTs, no link was provided to provide easy access to the data or models used in the study. There was no consistent naming of study types with a wide range of studies that could potentially be considered ISCTs. There is a clear need for community agreement on minimal reporting standards on patient demographics, accepted standards for ISCT cohort quality control, uncertainty quantification, and increased model and data sharing.</p>","PeriodicalId":74582,"journal":{"name":"Progress in biomedical engineering (Bristol, England)","volume":"5 3","pages":"032004"},"PeriodicalIF":7.7000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10286106/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Progress in biomedical engineering (Bristol, England)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1088/2516-1091/acdc71","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ENGINEERING, BIOMEDICAL","Score":null,"Total":0}
引用次数: 1
Abstract
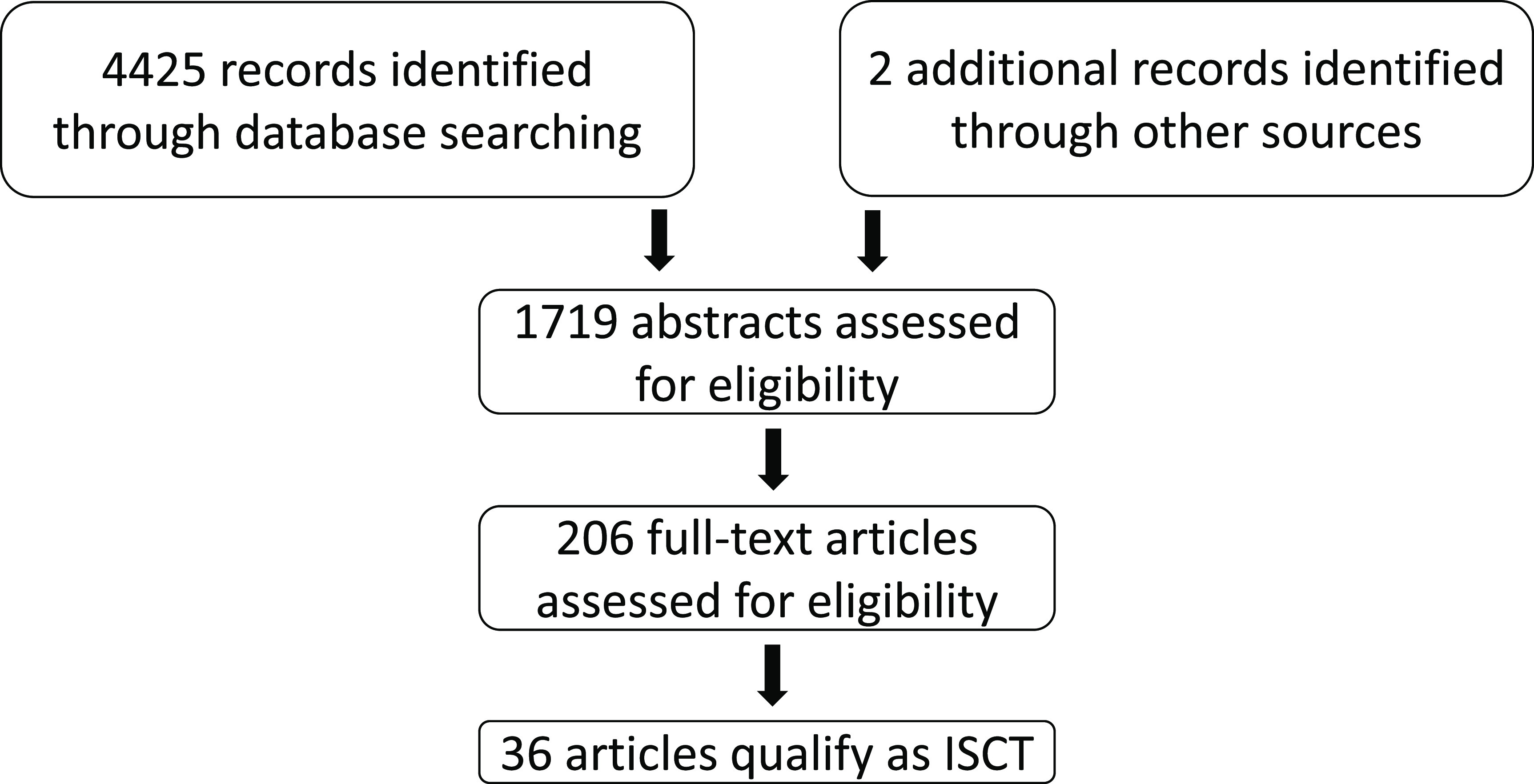
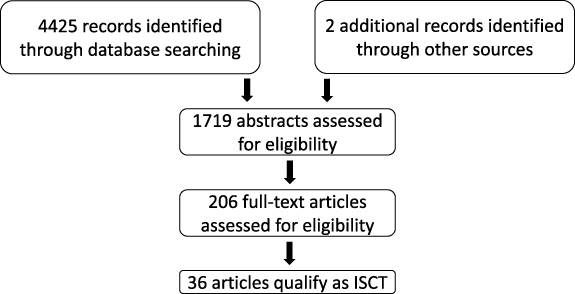
Computational models of the heart are now being used to assess the effectiveness and feasibility of interventions through in-silico clinical trials (ISCTs). As the adoption and acceptance of ISCTs increases, best practices for reporting the methodology and analysing the results will emerge. Focusing in the area of cardiology, we aim to evaluate the types of ISCTs, their analysis methods and their reporting standards. To this end, we conducted a systematic review of cardiac ISCTs over the period of 1 January 2012-1 January 2022, following the preferred reporting items for systematic reviews and meta-analysis (PRISMA). We considered cardiac ISCTs of human patient cohorts, and excluded studies of single individuals and those in which models were used to guide a procedure without comparing against a control group. We identified 36 publications that described cardiac ISCTs, with most of the studies coming from the US and the UK. In of the studies, a validation step was performed, although the specific type of validation varied between the studies. ANSYS FLUENT was the most commonly used software in of ISCTs. The specific software used was not reported in of the studies. Unlike clinical trials, we found a lack of consistent reporting of patient demographics, with of the studies not reporting them. Uncertainty quantification was limited, with sensitivity analysis performed in only of the studies. In of the ISCTs, no link was provided to provide easy access to the data or models used in the study. There was no consistent naming of study types with a wide range of studies that could potentially be considered ISCTs. There is a clear need for community agreement on minimal reporting standards on patient demographics, accepted standards for ISCT cohort quality control, uncertainty quantification, and increased model and data sharing.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
