{"title":"Factors associated with the author-reported cost-effectiveness threshold in high-income countries: systematic review and multivariable modelling.","authors":"Nicolas Boespflug, Jérôme Wittwer, Antoine Bénard","doi":"10.1007/s10198-023-01613-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The cost-effectiveness threshold (CET) is a key parameter to guide objective reimbursement decisions, yet very few countries have defined a reference CET, and there is no reference method for defining it. Our objective was to determine the factors explaining the author-reported CETs in the literature.</p><p><strong>Methods: </strong>Our systematic review targeted original articles referenced in EMBASE and published between 2010 and 2021. Selected studies had to use Quality-Adjusted Life-Year (QALY), and being conducted in high-income countries. Our explanatory variables were: estimated cost-effectiveness ratio (ICER), region of the world, source of funding, type of intervention, disease, year of publication, justification of the author-reported Cost-Effectiveness Threshold (ar-CET), economic perspective, and declaration of interest. Multivariable linear regression models implemented on R software were used, guided by a Directed Acyclic Graph.</p><p><strong>Results: </strong>Two hundred and fifty four studies were included. The mean ar-CET was €63,338/QALY (standard deviation (SD) 34,965) overall, and €37,748/QALY (SD 20,750) in studies conducted in the British Commonwealth. The ar-CET increased slightly with the ICER (+ 66€/QALY for each additional 10,000€/QALY in the ICER, 95% confidence interval (IC) [31-102], p < 0.001), was higher in the United States (+ 36,225€/QALY; IC [25,582; 46,869]) and Europe (+ 10,352€/QALY; IC [72; 20,631]) compared to the British Commonwealth (p < 0.001), and was higher when the ar-CET was not defined a priori (+ 22,393€/QALY; [5809; 38,876]) compared to state recommendations defined ar-CET (p < 0.001).</p><p><strong>Conclusions: </strong>Our results underline the virtuous role of state recommendations in the choice of a low and homogeneous CET. We also highlight the need to integrate the a priori justification of the CET into good publishing guidelines.</p>","PeriodicalId":51416,"journal":{"name":"European Journal of Health Economics","volume":" ","pages":"631-639"},"PeriodicalIF":3.0000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Health Economics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10198-023-01613-7","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/7/11 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: The cost-effectiveness threshold (CET) is a key parameter to guide objective reimbursement decisions, yet very few countries have defined a reference CET, and there is no reference method for defining it. Our objective was to determine the factors explaining the author-reported CETs in the literature.
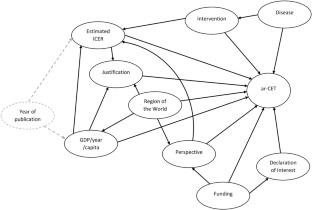
Methods: Our systematic review targeted original articles referenced in EMBASE and published between 2010 and 2021. Selected studies had to use Quality-Adjusted Life-Year (QALY), and being conducted in high-income countries. Our explanatory variables were: estimated cost-effectiveness ratio (ICER), region of the world, source of funding, type of intervention, disease, year of publication, justification of the author-reported Cost-Effectiveness Threshold (ar-CET), economic perspective, and declaration of interest. Multivariable linear regression models implemented on R software were used, guided by a Directed Acyclic Graph.
Results: Two hundred and fifty four studies were included. The mean ar-CET was €63,338/QALY (standard deviation (SD) 34,965) overall, and €37,748/QALY (SD 20,750) in studies conducted in the British Commonwealth. The ar-CET increased slightly with the ICER (+ 66€/QALY for each additional 10,000€/QALY in the ICER, 95% confidence interval (IC) [31-102], p < 0.001), was higher in the United States (+ 36,225€/QALY; IC [25,582; 46,869]) and Europe (+ 10,352€/QALY; IC [72; 20,631]) compared to the British Commonwealth (p < 0.001), and was higher when the ar-CET was not defined a priori (+ 22,393€/QALY; [5809; 38,876]) compared to state recommendations defined ar-CET (p < 0.001).
Conclusions: Our results underline the virtuous role of state recommendations in the choice of a low and homogeneous CET. We also highlight the need to integrate the a priori justification of the CET into good publishing guidelines.
期刊介绍:
The European Journal of Health Economics is a journal of Health Economics and associated disciplines. The growing demand for health economics and the introduction of new guidelines in various European countries were the motivation to generate a highly scientific and at the same time practice oriented journal considering the requirements of various health care systems in Europe. The international scientific board of opinion leaders guarantees high-quality, peer-reviewed publications as well as articles for pragmatic approaches in the field of health economics. We intend to cover all aspects of health economics:
• Basics of health economic approaches and methods
• Pharmacoeconomics
• Health Care Systems
• Pricing and Reimbursement Systems
• Quality-of-Life-Studies The editors reserve the right to reject manuscripts that do not comply with the above-mentioned requirements. The author will be held responsible for false statements or for failure to fulfill the above-mentioned requirements.
Officially cited as: Eur J Health Econ



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
