Claartje Meijs, M Louis Handoko, Gianluigi Savarese, Robin W M Vernooij, Ilonca Vaartjes, Amitava Banerjee, Stefan Koudstaal, Jasper J Brugts, Folkert W Asselbergs, Alicia Uijl
{"title":"Discovering Distinct Phenotypical Clusters in Heart Failure Across the Ejection Fraction Spectrum: a Systematic Review.","authors":"Claartje Meijs, M Louis Handoko, Gianluigi Savarese, Robin W M Vernooij, Ilonca Vaartjes, Amitava Banerjee, Stefan Koudstaal, Jasper J Brugts, Folkert W Asselbergs, Alicia Uijl","doi":"10.1007/s11897-023-00615-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Review purpose: </strong>This systematic review aims to summarise clustering studies in heart failure (HF) and guide future clinical trial design and implementation in routine clinical practice.</p><p><strong>Findings: </strong>34 studies were identified (n = 19 in HF with preserved ejection fraction (HFpEF)). There was significant heterogeneity invariables and techniques used. However, 149/165 described clusters could be assigned to one of nine phenotypes: 1) young, low comorbidity burden; 2) metabolic; 3) cardio-renal; 4) atrial fibrillation (AF); 5) elderly female AF; 6) hypertensive-comorbidity; 7) ischaemic-male; 8) valvular disease; and 9) devices. There was room for improvement on important methodological topics for all clustering studies such as external validation and transparency of the modelling process. The large overlap between the phenotypes of the clustering studies shows that clustering is a robust approach for discovering clinically distinct phenotypes. However, future studies should invest in a phenotype model that can be implemented in routine clinical practice and future clinical trial design. HF = heart failure, EF = ejection fraction, HFpEF = heart failure with preserved ejection fraction, HFrEF = heart failure with reduced ejection fraction, CKD = chronic kidney disease, AF = atrial fibrillation, IHD = ischaemic heart disease, CAD = coronary artery disease, ICD = implantable cardioverter-defibrillator, CRT = cardiac resynchronization therapy, NT-proBNP = N-terminal pro b-type natriuretic peptide, BMI = Body Mass Index, COPD = Chronic obstructive pulmonary disease.</p>","PeriodicalId":10830,"journal":{"name":"Current Heart Failure Reports","volume":" ","pages":"333-349"},"PeriodicalIF":3.4000,"publicationDate":"2023-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10589200/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current Heart Failure Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s11897-023-00615-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/7/21 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Review purpose: This systematic review aims to summarise clustering studies in heart failure (HF) and guide future clinical trial design and implementation in routine clinical practice.
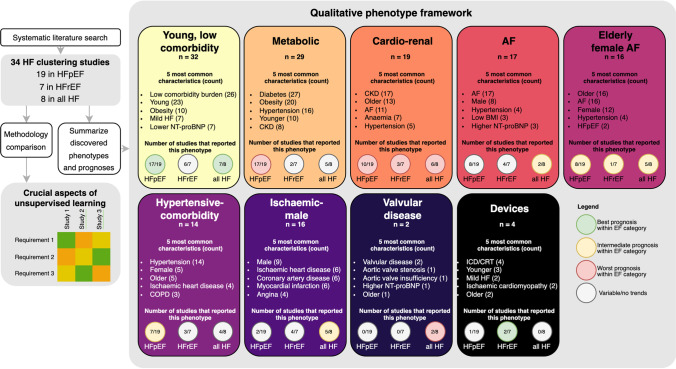
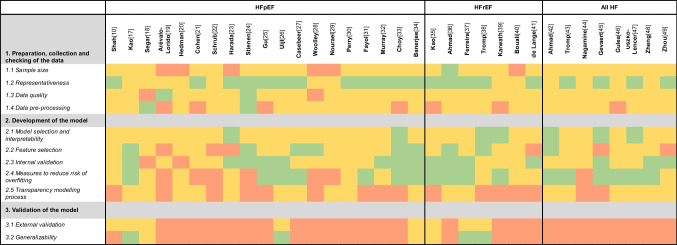
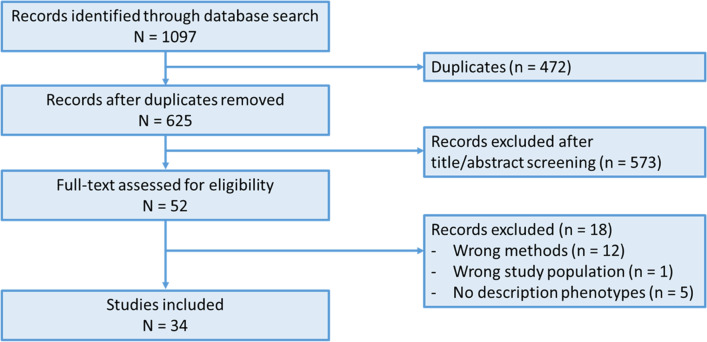
Findings: 34 studies were identified (n = 19 in HF with preserved ejection fraction (HFpEF)). There was significant heterogeneity invariables and techniques used. However, 149/165 described clusters could be assigned to one of nine phenotypes: 1) young, low comorbidity burden; 2) metabolic; 3) cardio-renal; 4) atrial fibrillation (AF); 5) elderly female AF; 6) hypertensive-comorbidity; 7) ischaemic-male; 8) valvular disease; and 9) devices. There was room for improvement on important methodological topics for all clustering studies such as external validation and transparency of the modelling process. The large overlap between the phenotypes of the clustering studies shows that clustering is a robust approach for discovering clinically distinct phenotypes. However, future studies should invest in a phenotype model that can be implemented in routine clinical practice and future clinical trial design. HF = heart failure, EF = ejection fraction, HFpEF = heart failure with preserved ejection fraction, HFrEF = heart failure with reduced ejection fraction, CKD = chronic kidney disease, AF = atrial fibrillation, IHD = ischaemic heart disease, CAD = coronary artery disease, ICD = implantable cardioverter-defibrillator, CRT = cardiac resynchronization therapy, NT-proBNP = N-terminal pro b-type natriuretic peptide, BMI = Body Mass Index, COPD = Chronic obstructive pulmonary disease.
期刊介绍:
This journal intends to provide clear, insightful, balanced contributions by international experts that review the most important, recently published clinical findings related to the diagnosis, treatment, management, and prevention of heart failure. We accomplish this aim by appointing international authorities to serve as Section Editors in key subject areas, such as investigative, pharmacologic, and nonpharmacologic therapies, pathophysiology, and prevention. Section Editors, in turn, select topics for which leading experts contribute comprehensive review articles that emphasize new developments and recently published papers of major importance, highlighted by annotated reference lists. An international Editorial Board reviews the annual table of contents, suggests articles of special interest to their country/region, and ensures that topics are current and include emerging research. Commentaries from well-known figures in the field are also provided.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
