{"title":"Etiologies and Predictors of 30-Day Readmission in Heart Failure: An Updated Analysis.","authors":"Akhil Jain, Shilpkumar Arora, Viral Patel, Maharshi Raval, Karnav Modi, Nirav Arora, Rupak Desai, Behnam Bozorgnia, Raphael Bonita","doi":"10.36628/ijhf.2023.0015","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>Readmissions in heart failure (HF), historically reported as 20%, contribute to significant patient morbidity and high financial cost to the healthcare system. The changing population landscape and risk factor dynamics mandate periodic epidemiologic reassessment of HF readmissions.</p><p><strong>Methods: </strong>National Readmission Database (NRD, 2019) was used to identify HF-related hospitalizations and evaluated for demographic, admission characteristics, and comorbidity differences between patients readmitted vs. those not readmitted at 30-days. Causes of readmission and predictors of all-cause, HF-specific, and non-HF-related readmissions were analyzed.</p><p><strong>Results: </strong>Of 48,971 HF patients, the readmitted cohort was younger (mean 67.4 vs. 68.9 years, p≤0.001), had higher proportion of males (56.3% vs. 53.7%), lowest income quartiles (33.3% vs. 28.9%), Charlson comorbidity index (CCI) ≥3 (61.7% vs. 52.8%), resource utilization including large bed-size hospitalizations, Medicaid enrollees, mean length of stay (6.2 vs. 5.4 days), and disposition to other facilities (23.9% vs. 20%) than non-readmitted. Readmission (30-day) rate was 21.2% (10,370) with cardiovascular causes in 50.3% (HF being the most common: 39%), and non-cardiac in 49.7%. Independent predictors for readmission were male sex, lower socioeconomic status, nonelective admissions, atrial fibrillation, chronic obstructive pulmonary disease, chronic kidney disease, anemia, and CCI ≥3. HF-specific readmissions were significantly associated with prior coronary artery disease and Medicaid enrollment.</p><p><strong>Conclusions: </strong>Our analysis revealed cardiac and noncardiac causes of readmission were equally common for 30-day readmissions in HF patients with HF itself being the most common etiology highlighting the importance of addressing the comorbidities, both cardiac and non-cardiac, to mitigate the risk of readmission.</p>","PeriodicalId":14058,"journal":{"name":"International Journal of Heart Failure","volume":"5 3","pages":"159-168"},"PeriodicalIF":0.0000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/68/d0/ijhf-5-159.PMC10406555.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Heart Failure","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36628/ijhf.2023.0015","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
Background and objectives: Readmissions in heart failure (HF), historically reported as 20%, contribute to significant patient morbidity and high financial cost to the healthcare system. The changing population landscape and risk factor dynamics mandate periodic epidemiologic reassessment of HF readmissions.
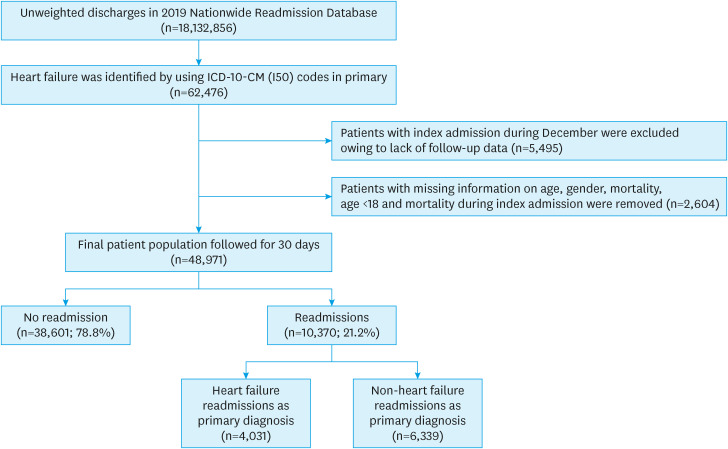
Methods: National Readmission Database (NRD, 2019) was used to identify HF-related hospitalizations and evaluated for demographic, admission characteristics, and comorbidity differences between patients readmitted vs. those not readmitted at 30-days. Causes of readmission and predictors of all-cause, HF-specific, and non-HF-related readmissions were analyzed.
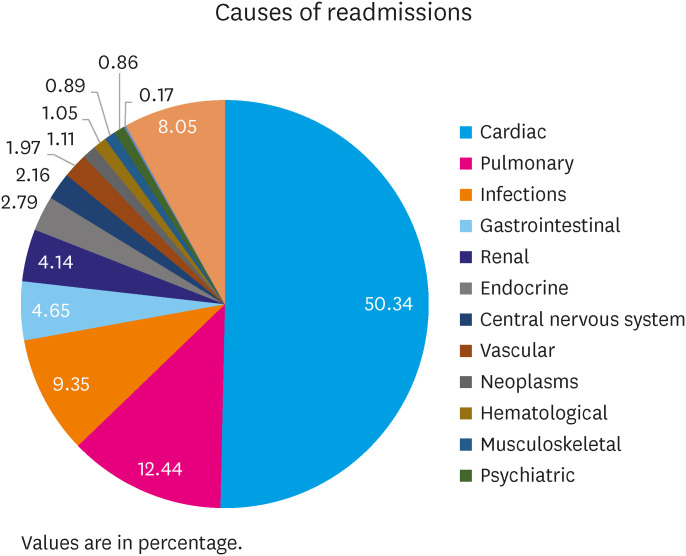
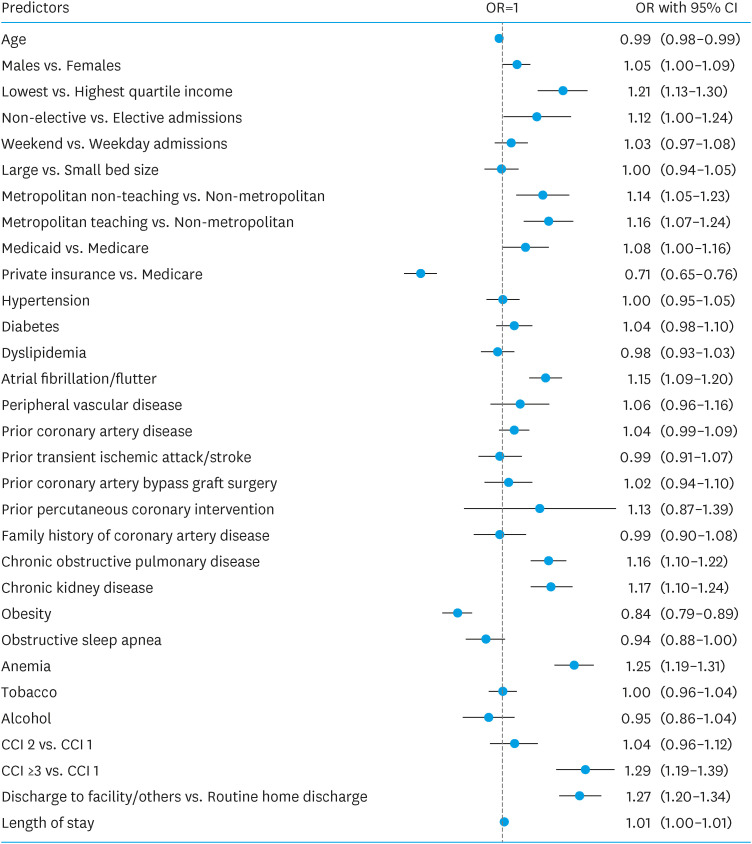
Results: Of 48,971 HF patients, the readmitted cohort was younger (mean 67.4 vs. 68.9 years, p≤0.001), had higher proportion of males (56.3% vs. 53.7%), lowest income quartiles (33.3% vs. 28.9%), Charlson comorbidity index (CCI) ≥3 (61.7% vs. 52.8%), resource utilization including large bed-size hospitalizations, Medicaid enrollees, mean length of stay (6.2 vs. 5.4 days), and disposition to other facilities (23.9% vs. 20%) than non-readmitted. Readmission (30-day) rate was 21.2% (10,370) with cardiovascular causes in 50.3% (HF being the most common: 39%), and non-cardiac in 49.7%. Independent predictors for readmission were male sex, lower socioeconomic status, nonelective admissions, atrial fibrillation, chronic obstructive pulmonary disease, chronic kidney disease, anemia, and CCI ≥3. HF-specific readmissions were significantly associated with prior coronary artery disease and Medicaid enrollment.
Conclusions: Our analysis revealed cardiac and noncardiac causes of readmission were equally common for 30-day readmissions in HF patients with HF itself being the most common etiology highlighting the importance of addressing the comorbidities, both cardiac and non-cardiac, to mitigate the risk of readmission.
背景和目的:心力衰竭(HF)的再入院率历来报道为20%,这导致了显著的患者发病率和医疗保健系统的高财务成本。不断变化的人口格局和危险因素动态要求定期对心衰再入院进行流行病学重新评估。方法:使用国家再入院数据库(NRD, 2019)来确定与hf相关的住院情况,并评估再入院患者与未再入院患者在30天内的人口学、入院特征和合并症差异。分析再入院的原因和全因再入院、hf特异性再入院和非hf相关再入院的预测因素。结果:在48971例HF患者中,再入院队列较年轻(平均67.4岁vs. 68.9岁,p≤0.001),男性比例较高(56.3% vs. 53.7%),收入最低(33.3% vs. 28.9%), Charlson合并症指数(CCI)≥3 (61.7% vs. 52.8%),资源利用率,包括大床住院,医疗补助登记,平均住院时间(6.2 vs. 5.4天),以及对其他设施的处置(23.9% vs. 20%)。再入院(30天)率为21.2%(10370例),其中心血管原因占50.3% (HF最常见:39%),非心脏原因占49.7%。再入院的独立预测因素为男性、较低的社会经济地位、非选择性入院、心房颤动、慢性阻塞性肺病、慢性肾病、贫血和CCI≥3。hf特异性再入院与既往冠状动脉疾病和医疗补助登记显著相关。结论:我们的分析显示,心脏和非心脏原因的再入院在HF患者30天再入院中同样常见,而HF本身是最常见的病因,强调了解决心脏和非心脏合并症的重要性,以降低再入院风险。


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
