{"title":"Spinal Rosai-Dorfman disease-a report of 2 cases and review of literature.","authors":"Saumyajit Basu, Rohan Gala, Kushal Gohil","doi":"10.1038/s41394-023-00600-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Rosai-Dorfman Disease (RDD) is a rare benign histiocytic disease that infrequently affects the spine. We report two cases of spinal RDD and review the relevant literature. This report addresses the various diagnostic dilemmas related to the evaluation of Spinal RDD and its treatment.</p><p><strong>Case presentation: </strong>Case 1: A 32-year-old male presented with low back pain and left anterior thigh for last 8 months. On examination, there was sensory diminution on inner aspects of the thigh with an absent left knee jerk. CT/MRI scans revealed an extradural lesion at L2/3 with neural compression. PET scan showed several hypermetabolic lesions in ribs, humerus, femur, and vertebrae. He underwent en bloc excision of the extradural mass with L2-3 pedicle screw-rod fixation and was later managed with chemotherapy. Case 2: A 42-year-old male presented with spastic paraparesis with urinary incontinence for the last 4 weeks. On examination, he had a neurological level of T6. MRI scan revealed a lesion in posterior elements of T6-7 compressing the spinal cord. He underwent T6-7 laminectomy with decompression. In both cases, the diagnosis was confirmed by histopathology and further managed by Hemato-oncologist. They both did well at 1-year follow-up with improvement in neurology.</p><p><strong>Discussion: </strong>Spinal RDD to date remains a large diagnostic dilemma with no pathognomonic clinical or radiological features; mimicking many osteolytic lesions in the spine. The diagnosis is purely histopathological and immunological. The lesion's complete surgical excision is the mainstay of treatment with a better prognosis and decreased chances of recurrences.</p>","PeriodicalId":22079,"journal":{"name":"Spinal Cord Series and Cases","volume":"9 1","pages":"36"},"PeriodicalIF":0.9000,"publicationDate":"2023-07-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10387076/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spinal Cord Series and Cases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1038/s41394-023-00600-7","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Rosai-Dorfman Disease (RDD) is a rare benign histiocytic disease that infrequently affects the spine. We report two cases of spinal RDD and review the relevant literature. This report addresses the various diagnostic dilemmas related to the evaluation of Spinal RDD and its treatment.
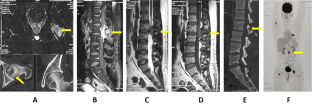
Case presentation: Case 1: A 32-year-old male presented with low back pain and left anterior thigh for last 8 months. On examination, there was sensory diminution on inner aspects of the thigh with an absent left knee jerk. CT/MRI scans revealed an extradural lesion at L2/3 with neural compression. PET scan showed several hypermetabolic lesions in ribs, humerus, femur, and vertebrae. He underwent en bloc excision of the extradural mass with L2-3 pedicle screw-rod fixation and was later managed with chemotherapy. Case 2: A 42-year-old male presented with spastic paraparesis with urinary incontinence for the last 4 weeks. On examination, he had a neurological level of T6. MRI scan revealed a lesion in posterior elements of T6-7 compressing the spinal cord. He underwent T6-7 laminectomy with decompression. In both cases, the diagnosis was confirmed by histopathology and further managed by Hemato-oncologist. They both did well at 1-year follow-up with improvement in neurology.
Discussion: Spinal RDD to date remains a large diagnostic dilemma with no pathognomonic clinical or radiological features; mimicking many osteolytic lesions in the spine. The diagnosis is purely histopathological and immunological. The lesion's complete surgical excision is the mainstay of treatment with a better prognosis and decreased chances of recurrences.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
