Tessa M.F. Watt MD, MSc , Alexander A. Brescia MD, MSc , Shannon L. Murray MSH , Liza M. Rosenbloom BA , Alexander Wisnielwski BS , David Burn PhD , Matthew A. Romano MD , Steven F. Bolling MD
{"title":"持续减少功能性二尖瓣反流是否影响生存?","authors":"Tessa M.F. Watt MD, MSc , Alexander A. Brescia MD, MSc , Shannon L. Murray MSH , Liza M. Rosenbloom BA , Alexander Wisnielwski BS , David Burn PhD , Matthew A. Romano MD , Steven F. Bolling MD","doi":"10.1053/j.semtcvs.2023.04.003","DOIUrl":null,"url":null,"abstract":"<div><p>Functional mitral regurgitation (FMR) is associated with increased mortality and has been considered a marker for advanced heart disease, yet the value of mitral valve repair (MVr) in this population remains unclear. This study aims to evaluate the impact of reducing FMR burden through surgical MVr on survival. Patients with severe FMR who underwent MVr with an undersized, complete, rigid, annuloplasty between 2004 and 2017 were assessed (n = 201). Patients were categorized based on grade of recurrent FMR (0-4). Time-to-event Kaplan-Meier estimations of freedom from death or reoperation were performed using the log-rank test. Cox proportional hazards models evaluated all-cause mortality and reported in hazards ratios (HR) and 95% confidence intervals (CI). Patients were categorized by postoperative recurrent FMR: 45% (91/201) of patients had grade 0, 29% (58/201) grade 1, 20% (40/201) grade 2, 2% (4/201) grade 3%, and 4% (8/201) grade 4. The cumulative incidence of reoperation with death as a competing risk was higher in patients with grades ≥3 recurrent FMR compared to grades ≤2 (44.6% vs 14.6%, subhazard ratio 3.69 [95% CI, 1.17-11.6]; <em>P</em> = 0.026). Overall freedom from death or reoperation was superior for recurrent FMR grades ≤2 compared to grades ≥3 (log-rank <em>P</em> < 0.001). Increasing recurrent FMR grade was independently associated with mortality (HR 1.30 [95% CI, 1.07-1.59] <em>P</em> = 0.009). Reduced postoperative FMR grade resulted in an incrementally lower risk of death or reoperation after MVr. These results suggest that achieving a durable reduction in FMR burden improves long-term survival.</p></div>","PeriodicalId":48592,"journal":{"name":"Seminars in Thoracic and Cardiovascular Surgery","volume":"36 1","pages":"Pages 37-46"},"PeriodicalIF":2.5000,"publicationDate":"2024-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S1043067923000874/pdfft?md5=706cec2afa2a6cc3d0e8caef22049958&pid=1-s2.0-S1043067923000874-main.pdf","citationCount":"0","resultStr":"{\"title\":\"Does Sustained Reduction of Functional Mitral Regurgitation Impact Survival?\",\"authors\":\"Tessa M.F. Watt MD, MSc , Alexander A. Brescia MD, MSc , Shannon L. Murray MSH , Liza M. Rosenbloom BA , Alexander Wisnielwski BS , David Burn PhD , Matthew A. Romano MD , Steven F. Bolling MD\",\"doi\":\"10.1053/j.semtcvs.2023.04.003\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><p>Functional mitral regurgitation (FMR) is associated with increased mortality and has been considered a marker for advanced heart disease, yet the value of mitral valve repair (MVr) in this population remains unclear. This study aims to evaluate the impact of reducing FMR burden through surgical MVr on survival. Patients with severe FMR who underwent MVr with an undersized, complete, rigid, annuloplasty between 2004 and 2017 were assessed (n = 201). Patients were categorized based on grade of recurrent FMR (0-4). Time-to-event Kaplan-Meier estimations of freedom from death or reoperation were performed using the log-rank test. Cox proportional hazards models evaluated all-cause mortality and reported in hazards ratios (HR) and 95% confidence intervals (CI). Patients were categorized by postoperative recurrent FMR: 45% (91/201) of patients had grade 0, 29% (58/201) grade 1, 20% (40/201) grade 2, 2% (4/201) grade 3%, and 4% (8/201) grade 4. The cumulative incidence of reoperation with death as a competing risk was higher in patients with grades ≥3 recurrent FMR compared to grades ≤2 (44.6% vs 14.6%, subhazard ratio 3.69 [95% CI, 1.17-11.6]; <em>P</em> = 0.026). Overall freedom from death or reoperation was superior for recurrent FMR grades ≤2 compared to grades ≥3 (log-rank <em>P</em> < 0.001). Increasing recurrent FMR grade was independently associated with mortality (HR 1.30 [95% CI, 1.07-1.59] <em>P</em> = 0.009). Reduced postoperative FMR grade resulted in an incrementally lower risk of death or reoperation after MVr. These results suggest that achieving a durable reduction in FMR burden improves long-term survival.</p></div>\",\"PeriodicalId\":48592,\"journal\":{\"name\":\"Seminars in Thoracic and Cardiovascular Surgery\",\"volume\":\"36 1\",\"pages\":\"Pages 37-46\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2024-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.sciencedirect.com/science/article/pii/S1043067923000874/pdfft?md5=706cec2afa2a6cc3d0e8caef22049958&pid=1-s2.0-S1043067923000874-main.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Seminars in Thoracic and Cardiovascular Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S1043067923000874\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/11/3 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Seminars in Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1043067923000874","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/11/3 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
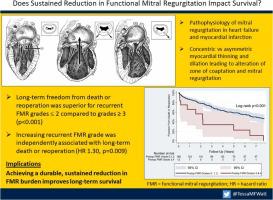
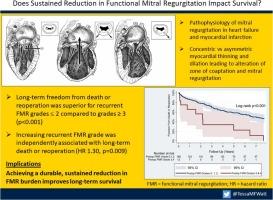
Does Sustained Reduction of Functional Mitral Regurgitation Impact Survival?
Functional mitral regurgitation (FMR) is associated with increased mortality and has been considered a marker for advanced heart disease, yet the value of mitral valve repair (MVr) in this population remains unclear. This study aims to evaluate the impact of reducing FMR burden through surgical MVr on survival. Patients with severe FMR who underwent MVr with an undersized, complete, rigid, annuloplasty between 2004 and 2017 were assessed (n = 201). Patients were categorized based on grade of recurrent FMR (0-4). Time-to-event Kaplan-Meier estimations of freedom from death or reoperation were performed using the log-rank test. Cox proportional hazards models evaluated all-cause mortality and reported in hazards ratios (HR) and 95% confidence intervals (CI). Patients were categorized by postoperative recurrent FMR: 45% (91/201) of patients had grade 0, 29% (58/201) grade 1, 20% (40/201) grade 2, 2% (4/201) grade 3%, and 4% (8/201) grade 4. The cumulative incidence of reoperation with death as a competing risk was higher in patients with grades ≥3 recurrent FMR compared to grades ≤2 (44.6% vs 14.6%, subhazard ratio 3.69 [95% CI, 1.17-11.6]; P = 0.026). Overall freedom from death or reoperation was superior for recurrent FMR grades ≤2 compared to grades ≥3 (log-rank P < 0.001). Increasing recurrent FMR grade was independently associated with mortality (HR 1.30 [95% CI, 1.07-1.59] P = 0.009). Reduced postoperative FMR grade resulted in an incrementally lower risk of death or reoperation after MVr. These results suggest that achieving a durable reduction in FMR burden improves long-term survival.
期刊介绍:
Seminars in Thoracic and Cardiovascular Surgery is devoted to providing a forum for cardiothoracic surgeons to disseminate and discuss important new information and to gain insight into unresolved areas of question in the specialty. Each issue presents readers with a selection of original peer-reviewed articles accompanied by editorial commentary from specialists in the field. In addition, readers are offered valuable invited articles: State of Views editorials and Current Readings highlighting the latest contributions on central or controversial issues. Another prized feature is expert roundtable discussions in which experts debate critical questions for cardiothoracic treatment and care. Seminars is an invitation-only publication that receives original submissions transferred ONLY from its sister publication, The Journal of Thoracic and Cardiovascular Surgery. As we continue to expand the reach of the Journal, we will explore the possibility of accepting unsolicited manuscripts in the future.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
