Elis Susilawati, Jutti Levita, Yasmiwar Susilawati, Sri Adi Sumiwi
{"title":"二甲双胍、磺脲和噻唑烷二酮治疗2型糖尿病的病例报告综述。","authors":"Elis Susilawati, Jutti Levita, Yasmiwar Susilawati, Sri Adi Sumiwi","doi":"10.3390/medsci11030050","DOIUrl":null,"url":null,"abstract":"<p><p>Type 2 diabetes mellitus (T2DM) is the world's most common metabolic disease. The development of T2DM is mainly caused by a combination of two factors: the failure of insulin secretion by the pancreatic β-cells and the inability of insulin-sensitive tissues to respond to insulin (insulin resistance); therefore, the disease is indicated by a chronic increase in blood glucose. T2DM patients can be treated with mono- or combined therapy using oral antidiabetic drugs and insulin-replaced agents; however, the medication often leads to various discomforts, such as abdominal pain, diarrhea or constipation, nausea and vomiting, and hypersensitivity reactions. A biguanide drug, metformin, has been used as a first-line drug to reduce blood sugar levels. Sulfonylureas work by blocking the ATP-sensitive potassium channel, directly inducing the release of insulin from pancreatic β-cells and thus decreasing blood glucose concentrations. However, the risk of the failure of sulfonylurea as a monotherapy agent is greater than that of metformin or rosiglitazone (a thiazolidinedione drug). Sulfonylureas are used as the first-line drug of choice for DM patients who cannot tolerate metformin therapy. Other antidiabetic drugs, thiazolidinediones, work by activating the peroxisome proliferator-activated receptor gamma (PPARγ), decreasing the IR level, and increasing the response of β-cells towards the glucose level. However, thiazolidines may increase the risk of cardiovascular disease, weight gain, water retention, and edema. This review article aims to discuss case reports on the use of metformin, sulfonylureas, and thiazolidinediones in DM patients. The literature search was conducted on the PubMed database using the keywords 'metformin OR sulfonylureas OR thiazolidinediones AND case reports', filtered to 'free full text', 'case reports', and '10 years publication date'. In some patients, metformin may affect sleep quality and, in rare cases, leads to the occurrence of lactate acidosis; thus, patients taking this drug should be monitored for their kidney status, plasma pH, and plasma metformin level. Sulfonylureas and TZDs may cause a higher risk of hypoglycemia and weight gain or edema due to fluid retention. TZDs may be associated with risks of cardiovascular events in patients with concomitant T2DM and chronic obstructive pulmonary disease. Therefore, patients taking these drugs should be closely monitored for adverse effects.</p>","PeriodicalId":74152,"journal":{"name":"Medical sciences (Basel, Switzerland)","volume":"11 3","pages":""},"PeriodicalIF":4.4000,"publicationDate":"2023-08-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10443323/pdf/","citationCount":"2","resultStr":"{\"title\":\"Review of the Case Reports on Metformin, Sulfonylurea, and Thiazolidinedione Therapies in Type 2 Diabetes Mellitus Patients.\",\"authors\":\"Elis Susilawati, Jutti Levita, Yasmiwar Susilawati, Sri Adi Sumiwi\",\"doi\":\"10.3390/medsci11030050\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Type 2 diabetes mellitus (T2DM) is the world's most common metabolic disease. The development of T2DM is mainly caused by a combination of two factors: the failure of insulin secretion by the pancreatic β-cells and the inability of insulin-sensitive tissues to respond to insulin (insulin resistance); therefore, the disease is indicated by a chronic increase in blood glucose. T2DM patients can be treated with mono- or combined therapy using oral antidiabetic drugs and insulin-replaced agents; however, the medication often leads to various discomforts, such as abdominal pain, diarrhea or constipation, nausea and vomiting, and hypersensitivity reactions. A biguanide drug, metformin, has been used as a first-line drug to reduce blood sugar levels. Sulfonylureas work by blocking the ATP-sensitive potassium channel, directly inducing the release of insulin from pancreatic β-cells and thus decreasing blood glucose concentrations. However, the risk of the failure of sulfonylurea as a monotherapy agent is greater than that of metformin or rosiglitazone (a thiazolidinedione drug). Sulfonylureas are used as the first-line drug of choice for DM patients who cannot tolerate metformin therapy. Other antidiabetic drugs, thiazolidinediones, work by activating the peroxisome proliferator-activated receptor gamma (PPARγ), decreasing the IR level, and increasing the response of β-cells towards the glucose level. However, thiazolidines may increase the risk of cardiovascular disease, weight gain, water retention, and edema. This review article aims to discuss case reports on the use of metformin, sulfonylureas, and thiazolidinediones in DM patients. The literature search was conducted on the PubMed database using the keywords 'metformin OR sulfonylureas OR thiazolidinediones AND case reports', filtered to 'free full text', 'case reports', and '10 years publication date'. In some patients, metformin may affect sleep quality and, in rare cases, leads to the occurrence of lactate acidosis; thus, patients taking this drug should be monitored for their kidney status, plasma pH, and plasma metformin level. Sulfonylureas and TZDs may cause a higher risk of hypoglycemia and weight gain or edema due to fluid retention. TZDs may be associated with risks of cardiovascular events in patients with concomitant T2DM and chronic obstructive pulmonary disease. Therefore, patients taking these drugs should be closely monitored for adverse effects.</p>\",\"PeriodicalId\":74152,\"journal\":{\"name\":\"Medical sciences (Basel, Switzerland)\",\"volume\":\"11 3\",\"pages\":\"\"},\"PeriodicalIF\":4.4000,\"publicationDate\":\"2023-08-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10443323/pdf/\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Medical sciences (Basel, Switzerland)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3390/medsci11030050\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical sciences (Basel, Switzerland)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/medsci11030050","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 2
摘要
2型糖尿病(T2DM)是世界上最常见的代谢疾病。2型糖尿病的发生主要是由两种因素共同作用引起的:胰腺β细胞分泌胰岛素的失败和胰岛素敏感组织对胰岛素的反应(胰岛素抵抗)的丧失;因此,该病表现为血糖的慢性升高。2型糖尿病患者可采用口服降糖药和胰岛素替代药物的单一或联合治疗;然而,药物经常导致各种不适,如腹痛,腹泻或便秘,恶心和呕吐,以及过敏反应。双胍类药物二甲双胍已被用作降低血糖水平的一线药物。磺脲类药物通过阻断atp敏感的钾通道起作用,直接诱导胰腺β细胞释放胰岛素,从而降低血糖浓度。然而,磺脲类单药治疗失败的风险大于二甲双胍或罗格列酮(一种噻唑烷二酮类药物)。磺脲类药物被用作不能耐受二甲双胍治疗的糖尿病患者的首选一线药物。其他抗糖尿病药物,噻唑烷二酮类,通过激活过氧化物酶体增殖体激活受体γ (PPARγ),降低IR水平,增加β细胞对葡萄糖水平的反应。然而,噻唑烷类可能增加心血管疾病、体重增加、水潴留和水肿的风险。这篇综述文章旨在讨论二甲双胍、磺脲类药物和噻唑烷二酮类药物在糖尿病患者中的应用。在PubMed数据库中使用关键词“metformin OR sulfonylureas OR thiazolidinediones AND case reports”进行文献检索,过滤为“免费全文”、“病例报告”和“10年出版日期”。在一些患者中,二甲双胍可能影响睡眠质量,并在极少数情况下导致乳酸酸中毒的发生;因此,服用该药的患者应监测其肾脏状况、血浆pH值和血浆二甲双胍水平。磺脲类药物和tzd类药物可能导致低血糖和体重增加或因液体潴留造成水肿的风险更高。T2DM合并慢性阻塞性肺疾病患者TZDs可能与心血管事件风险相关。因此,应密切监测患者服用这些药物的不良反应。
Review of the Case Reports on Metformin, Sulfonylurea, and Thiazolidinedione Therapies in Type 2 Diabetes Mellitus Patients.
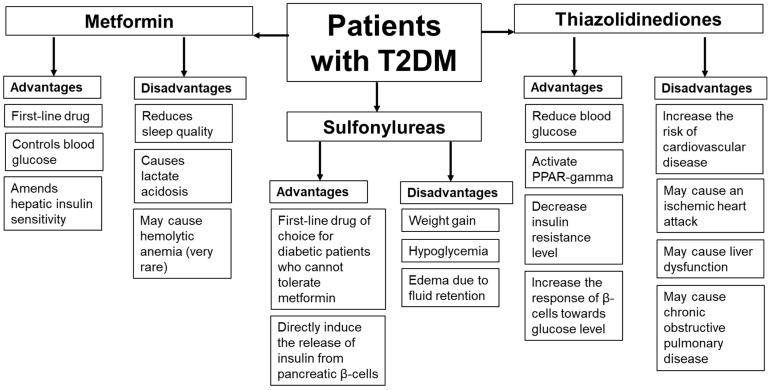
Type 2 diabetes mellitus (T2DM) is the world's most common metabolic disease. The development of T2DM is mainly caused by a combination of two factors: the failure of insulin secretion by the pancreatic β-cells and the inability of insulin-sensitive tissues to respond to insulin (insulin resistance); therefore, the disease is indicated by a chronic increase in blood glucose. T2DM patients can be treated with mono- or combined therapy using oral antidiabetic drugs and insulin-replaced agents; however, the medication often leads to various discomforts, such as abdominal pain, diarrhea or constipation, nausea and vomiting, and hypersensitivity reactions. A biguanide drug, metformin, has been used as a first-line drug to reduce blood sugar levels. Sulfonylureas work by blocking the ATP-sensitive potassium channel, directly inducing the release of insulin from pancreatic β-cells and thus decreasing blood glucose concentrations. However, the risk of the failure of sulfonylurea as a monotherapy agent is greater than that of metformin or rosiglitazone (a thiazolidinedione drug). Sulfonylureas are used as the first-line drug of choice for DM patients who cannot tolerate metformin therapy. Other antidiabetic drugs, thiazolidinediones, work by activating the peroxisome proliferator-activated receptor gamma (PPARγ), decreasing the IR level, and increasing the response of β-cells towards the glucose level. However, thiazolidines may increase the risk of cardiovascular disease, weight gain, water retention, and edema. This review article aims to discuss case reports on the use of metformin, sulfonylureas, and thiazolidinediones in DM patients. The literature search was conducted on the PubMed database using the keywords 'metformin OR sulfonylureas OR thiazolidinediones AND case reports', filtered to 'free full text', 'case reports', and '10 years publication date'. In some patients, metformin may affect sleep quality and, in rare cases, leads to the occurrence of lactate acidosis; thus, patients taking this drug should be monitored for their kidney status, plasma pH, and plasma metformin level. Sulfonylureas and TZDs may cause a higher risk of hypoglycemia and weight gain or edema due to fluid retention. TZDs may be associated with risks of cardiovascular events in patients with concomitant T2DM and chronic obstructive pulmonary disease. Therefore, patients taking these drugs should be closely monitored for adverse effects.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
