Yanping Du, Huaping Zhang, Zhiyi Ma, Jun Liu, Zhiyong Wang, Meixia Lin, Fayu Ni, Xi Li, Hui Tan, Shifan Tan, Yanling Chai, Xiangzhu Zhong
{"title":"慢性阻塞性肺疾病急性加重期患者的高流量鼻吸氧与无创通气:随机对照试验的荟萃分析","authors":"Yanping Du, Huaping Zhang, Zhiyi Ma, Jun Liu, Zhiyong Wang, Meixia Lin, Fayu Ni, Xi Li, Hui Tan, Shifan Tan, Yanling Chai, Xiangzhu Zhong","doi":"10.1155/2023/7707010","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>High-flow nasal cannula (HFNC) can be used in stable chronic obstructive pulmonary disease (COPD) patients, but the effect of HFNC on clinical outcomes in patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD) is still uncertain.</p><p><strong>Methods: </strong>We searched electronic literature databases for randomized controlled trials (RCTs) comparing HFNC with noninvasive ventilation (NIV) in hypercapnic patients with AECOPD. The primary endpoint of this meta-analysis was PaCO<sub>2</sub>, PaO<sub>2,</sub> and SpO<sub>2</sub>. The secondary outcomes were the respiratory rate, mortality, complications, and intubation rate.</p><p><strong>Results: </strong>We included 7 RCTs with a total of 481 patients. There were no significant differences on measures of PaCO<sub>2</sub> (MD = -0.42, 95%CI -3.60 to 2.75, <i>Z</i> = 0.26, and <i>P</i> = 0.79), PaO<sub>2</sub> (MD = -1.36, 95%CI -4.69 to 1.97, <i>Z</i> = 0.80, and <i>P</i> = 0.42), and SpO<sub>2</sub> (MD = -0.78, 95%CI -1.67 to 0.11, <i>Z</i> = 1.72, <i>P</i> = 0.08) between the HFNC group and the NIV group. There was no significant difference in measures of the mortality and intubation rate between the HFNC group (OR = 0.72, 95%CI 0.30 to 1.69, <i>Z</i> = 0.76, and <i>P</i> = 0.44) and the NIV group (OR = 2.38, 95%CI 0.49 to 11.50, <i>Z</i> = 1.08, and <i>P</i> = 0.28), respectively. But the respiratory rate in the HFNC group was lower than that in the NIV group (MD = -1.13, 95%CI -2.13 to -0.14, <i>Z</i> = 2.23, and <i>P</i> = 0.03), and fewer complications were found in the HFNC group (OR = 0.26, 95%CI 0.14 to 0.47, <i>Z</i> = 4.46, and <i>P</i> < 0.00001).</p><p><strong>Conclusion: </strong>NIV was noninferior to HFNC in decreasing PaCO<sub>2</sub> and increasing PaO<sub>2</sub> and SpO<sub>2</sub>. Similarly, the mortality and intubation rate was similar among the two groups. The respiratory rate and complications were inferior in the AECOPD group treated with HFNC.</p>","PeriodicalId":9416,"journal":{"name":"Canadian respiratory journal","volume":"2023 ","pages":"7707010"},"PeriodicalIF":2.1000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10328729/pdf/","citationCount":"1","resultStr":"{\"title\":\"High-Flow Nasal Oxygen versus Noninvasive Ventilation in Acute Exacerbation of Chronic Obstructive Pulmonary Disease Patients: A Meta-Analysis of Randomized Controlled Trials.\",\"authors\":\"Yanping Du, Huaping Zhang, Zhiyi Ma, Jun Liu, Zhiyong Wang, Meixia Lin, Fayu Ni, Xi Li, Hui Tan, Shifan Tan, Yanling Chai, Xiangzhu Zhong\",\"doi\":\"10.1155/2023/7707010\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>High-flow nasal cannula (HFNC) can be used in stable chronic obstructive pulmonary disease (COPD) patients, but the effect of HFNC on clinical outcomes in patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD) is still uncertain.</p><p><strong>Methods: </strong>We searched electronic literature databases for randomized controlled trials (RCTs) comparing HFNC with noninvasive ventilation (NIV) in hypercapnic patients with AECOPD. The primary endpoint of this meta-analysis was PaCO<sub>2</sub>, PaO<sub>2,</sub> and SpO<sub>2</sub>. The secondary outcomes were the respiratory rate, mortality, complications, and intubation rate.</p><p><strong>Results: </strong>We included 7 RCTs with a total of 481 patients. There were no significant differences on measures of PaCO<sub>2</sub> (MD = -0.42, 95%CI -3.60 to 2.75, <i>Z</i> = 0.26, and <i>P</i> = 0.79), PaO<sub>2</sub> (MD = -1.36, 95%CI -4.69 to 1.97, <i>Z</i> = 0.80, and <i>P</i> = 0.42), and SpO<sub>2</sub> (MD = -0.78, 95%CI -1.67 to 0.11, <i>Z</i> = 1.72, <i>P</i> = 0.08) between the HFNC group and the NIV group. There was no significant difference in measures of the mortality and intubation rate between the HFNC group (OR = 0.72, 95%CI 0.30 to 1.69, <i>Z</i> = 0.76, and <i>P</i> = 0.44) and the NIV group (OR = 2.38, 95%CI 0.49 to 11.50, <i>Z</i> = 1.08, and <i>P</i> = 0.28), respectively. But the respiratory rate in the HFNC group was lower than that in the NIV group (MD = -1.13, 95%CI -2.13 to -0.14, <i>Z</i> = 2.23, and <i>P</i> = 0.03), and fewer complications were found in the HFNC group (OR = 0.26, 95%CI 0.14 to 0.47, <i>Z</i> = 4.46, and <i>P</i> < 0.00001).</p><p><strong>Conclusion: </strong>NIV was noninferior to HFNC in decreasing PaCO<sub>2</sub> and increasing PaO<sub>2</sub> and SpO<sub>2</sub>. Similarly, the mortality and intubation rate was similar among the two groups. The respiratory rate and complications were inferior in the AECOPD group treated with HFNC.</p>\",\"PeriodicalId\":9416,\"journal\":{\"name\":\"Canadian respiratory journal\",\"volume\":\"2023 \",\"pages\":\"7707010\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10328729/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Canadian respiratory journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1155/2023/7707010\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian respiratory journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/2023/7707010","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 1
摘要
背景:高流量鼻插管(HFNC)可用于稳定期慢性阻塞性肺疾病(COPD)患者,但HFNC对慢性阻塞性肺疾病急性加重期(AECOPD)患者临床结局的影响尚不明确。方法:我们检索电子文献数据库,比较HFNC与无创通气(NIV)治疗AECOPD高碳酸血症患者的随机对照试验(rct)。这项荟萃分析的主要终点是PaCO2、PaO2和SpO2。次要结局为呼吸频率、死亡率、并发症和插管率。结果:我们纳入了7项随机对照试验,共481例患者。HFNC组与NIV组PaCO2 (MD = -0.42, 95%CI -3.60 ~ 2.75, Z = 0.26, P = 0.79)、PaO2 (MD = -1.36, 95%CI -4.69 ~ 1.97, Z = 0.80, P = 0.42)、SpO2 (MD = -0.78, 95%CI -1.67 ~ 0.11, Z = 1.72, P = 0.08)指标无显著差异。HFNC组(OR = 0.72, 95%CI 0.30 ~ 1.69, Z = 0.76, P = 0.44)与NIV组(OR = 2.38, 95%CI 0.49 ~ 11.50, Z = 1.08, P = 0.28)的死亡率和插管率指标无显著差异。但HFNC组呼吸频率低于NIV组(MD = -1.13, 95%CI为-2.13 ~ -0.14,Z = 2.23, P = 0.03),并发症发生率低于NIV组(OR = 0.26, 95%CI为0.14 ~ 0.47,Z = 4.46, P)。结论:NIV在降低PaCO2、升高PaO2和SpO2方面不低于HFNC组。同样,两组的死亡率和插管率相似。HFNC治疗AECOPD组呼吸频率及并发症均较低。
High-Flow Nasal Oxygen versus Noninvasive Ventilation in Acute Exacerbation of Chronic Obstructive Pulmonary Disease Patients: A Meta-Analysis of Randomized Controlled Trials.
Background: High-flow nasal cannula (HFNC) can be used in stable chronic obstructive pulmonary disease (COPD) patients, but the effect of HFNC on clinical outcomes in patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD) is still uncertain.
Methods: We searched electronic literature databases for randomized controlled trials (RCTs) comparing HFNC with noninvasive ventilation (NIV) in hypercapnic patients with AECOPD. The primary endpoint of this meta-analysis was PaCO2, PaO2, and SpO2. The secondary outcomes were the respiratory rate, mortality, complications, and intubation rate.
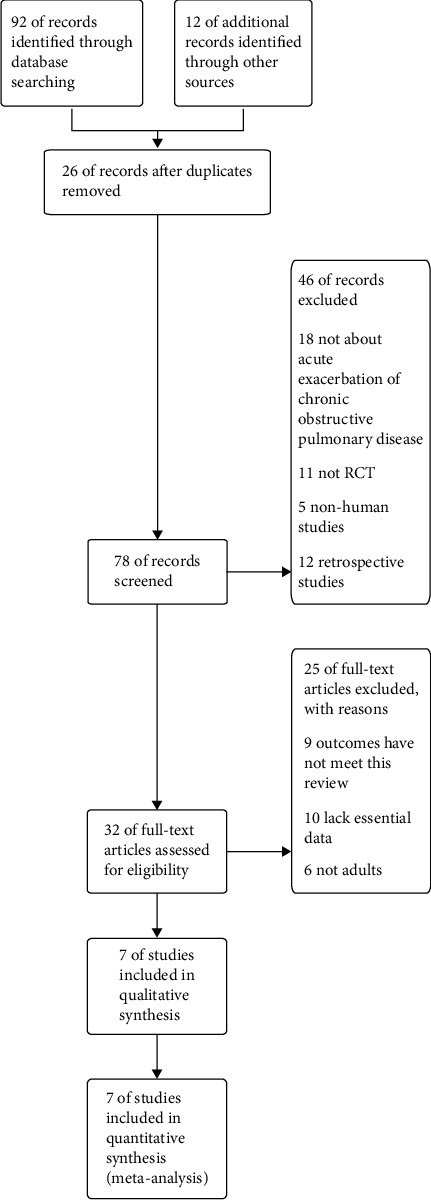
Results: We included 7 RCTs with a total of 481 patients. There were no significant differences on measures of PaCO2 (MD = -0.42, 95%CI -3.60 to 2.75, Z = 0.26, and P = 0.79), PaO2 (MD = -1.36, 95%CI -4.69 to 1.97, Z = 0.80, and P = 0.42), and SpO2 (MD = -0.78, 95%CI -1.67 to 0.11, Z = 1.72, P = 0.08) between the HFNC group and the NIV group. There was no significant difference in measures of the mortality and intubation rate between the HFNC group (OR = 0.72, 95%CI 0.30 to 1.69, Z = 0.76, and P = 0.44) and the NIV group (OR = 2.38, 95%CI 0.49 to 11.50, Z = 1.08, and P = 0.28), respectively. But the respiratory rate in the HFNC group was lower than that in the NIV group (MD = -1.13, 95%CI -2.13 to -0.14, Z = 2.23, and P = 0.03), and fewer complications were found in the HFNC group (OR = 0.26, 95%CI 0.14 to 0.47, Z = 4.46, and P < 0.00001).
Conclusion: NIV was noninferior to HFNC in decreasing PaCO2 and increasing PaO2 and SpO2. Similarly, the mortality and intubation rate was similar among the two groups. The respiratory rate and complications were inferior in the AECOPD group treated with HFNC.
期刊介绍:
Canadian Respiratory Journal is a peer-reviewed, Open Access journal that aims to provide a multidisciplinary forum for research in all areas of respiratory medicine. The journal publishes original research articles, review articles, and clinical studies related to asthma, allergy, COPD, non-invasive ventilation, therapeutic intervention, lung cancer, airway and lung infections, as well as any other respiratory diseases.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
