Brendan F Judy, Jovanna A Tracz, Jordina Rincon-Torroella, A Karim Ahmed, Timothy F Witham
{"title":"减轻非卧床病人的颈胸椎病:当牵引失败时。","authors":"Brendan F Judy, Jovanna A Tracz, Jordina Rincon-Torroella, A Karim Ahmed, Timothy F Witham","doi":"10.1038/s41394-023-00604-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Cervical spondyloptosis is a rare complication of high-energy trauma which often results in significant patient morbidity and mortality. The authors present a case of spondyloptosis of C7 over T1 with minimal radicular symptoms and otherwise complete spinal cord sparing. This case highlights the surgical challenges faced with cervical spondyloptosis and the techniques used when traction fails.</p><p><strong>Case presentation: </strong>A 21-year-old man with no significant past medical history presented after a high-speed motor vehicle collision with cervicothoracic pain and mild hand grip weakness in addition to numbness of the fourth and fifth digits bilaterally (American Spinal Injury Association Impairment Scale Grade D). Computed tomography imaging revealed spondyloptosis of C7 over T1, a fracture of the C2 vertebral body, and a burst fracture of C3. To relieve spinal cord compression and restore sagittal realignment, closed reduction was attempted, however this resulted in perching of the bilateral C7-T1 facets, leading to an open posterior approach. The patient underwent C7 laminectomy, bilateral C7-T1 facetectomy, and manual reduction using a Mayfield skull clamp followed by C2-T3 fixation. Postoperatively, pain was diminished, sensory disturbances were resolved and the patient was otherwise neurologically stable.</p><p><strong>Discussion: </strong>There is a role for closed traction for reduction of cervical spondyloptosis, however, its role is debated especially when the patient is predominately neurologically intact. In this setting, the spine surgeon may be required to change traction and operative strategies in order to minimize potentially harmful manipulation while restoring sagittal realignment and stabilizing the spine for preservation of neurological function.</p>","PeriodicalId":22079,"journal":{"name":"Spinal Cord Series and Cases","volume":"9 1","pages":"46"},"PeriodicalIF":0.9000,"publicationDate":"2023-09-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10477183/pdf/","citationCount":"0","resultStr":"{\"title\":\"Reduction of cervicothoracic spondyloptosis in an ambulatory patient: when traction fails.\",\"authors\":\"Brendan F Judy, Jovanna A Tracz, Jordina Rincon-Torroella, A Karim Ahmed, Timothy F Witham\",\"doi\":\"10.1038/s41394-023-00604-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Cervical spondyloptosis is a rare complication of high-energy trauma which often results in significant patient morbidity and mortality. The authors present a case of spondyloptosis of C7 over T1 with minimal radicular symptoms and otherwise complete spinal cord sparing. This case highlights the surgical challenges faced with cervical spondyloptosis and the techniques used when traction fails.</p><p><strong>Case presentation: </strong>A 21-year-old man with no significant past medical history presented after a high-speed motor vehicle collision with cervicothoracic pain and mild hand grip weakness in addition to numbness of the fourth and fifth digits bilaterally (American Spinal Injury Association Impairment Scale Grade D). Computed tomography imaging revealed spondyloptosis of C7 over T1, a fracture of the C2 vertebral body, and a burst fracture of C3. To relieve spinal cord compression and restore sagittal realignment, closed reduction was attempted, however this resulted in perching of the bilateral C7-T1 facets, leading to an open posterior approach. The patient underwent C7 laminectomy, bilateral C7-T1 facetectomy, and manual reduction using a Mayfield skull clamp followed by C2-T3 fixation. Postoperatively, pain was diminished, sensory disturbances were resolved and the patient was otherwise neurologically stable.</p><p><strong>Discussion: </strong>There is a role for closed traction for reduction of cervical spondyloptosis, however, its role is debated especially when the patient is predominately neurologically intact. In this setting, the spine surgeon may be required to change traction and operative strategies in order to minimize potentially harmful manipulation while restoring sagittal realignment and stabilizing the spine for preservation of neurological function.</p>\",\"PeriodicalId\":22079,\"journal\":{\"name\":\"Spinal Cord Series and Cases\",\"volume\":\"9 1\",\"pages\":\"46\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2023-09-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10477183/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Spinal Cord Series and Cases\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1038/s41394-023-00604-3\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spinal Cord Series and Cases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1038/s41394-023-00604-3","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Reduction of cervicothoracic spondyloptosis in an ambulatory patient: when traction fails.
Introduction: Cervical spondyloptosis is a rare complication of high-energy trauma which often results in significant patient morbidity and mortality. The authors present a case of spondyloptosis of C7 over T1 with minimal radicular symptoms and otherwise complete spinal cord sparing. This case highlights the surgical challenges faced with cervical spondyloptosis and the techniques used when traction fails.
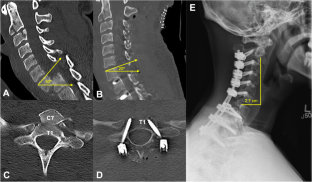
Case presentation: A 21-year-old man with no significant past medical history presented after a high-speed motor vehicle collision with cervicothoracic pain and mild hand grip weakness in addition to numbness of the fourth and fifth digits bilaterally (American Spinal Injury Association Impairment Scale Grade D). Computed tomography imaging revealed spondyloptosis of C7 over T1, a fracture of the C2 vertebral body, and a burst fracture of C3. To relieve spinal cord compression and restore sagittal realignment, closed reduction was attempted, however this resulted in perching of the bilateral C7-T1 facets, leading to an open posterior approach. The patient underwent C7 laminectomy, bilateral C7-T1 facetectomy, and manual reduction using a Mayfield skull clamp followed by C2-T3 fixation. Postoperatively, pain was diminished, sensory disturbances were resolved and the patient was otherwise neurologically stable.
Discussion: There is a role for closed traction for reduction of cervical spondyloptosis, however, its role is debated especially when the patient is predominately neurologically intact. In this setting, the spine surgeon may be required to change traction and operative strategies in order to minimize potentially harmful manipulation while restoring sagittal realignment and stabilizing the spine for preservation of neurological function.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
