Khawaja M. Talha, Ambarish Pandey, Marat Fudim, Javed Butler, Stefan D. Anker, Muhammad Shahzeb Khan
{"title":"虚弱和心力衰竭:最新综述。","authors":"Khawaja M. Talha, Ambarish Pandey, Marat Fudim, Javed Butler, Stefan D. Anker, Muhammad Shahzeb Khan","doi":"10.1002/jcsm.13306","DOIUrl":null,"url":null,"abstract":"<p>At least half of all patients with heart failure (HF) are affected by frailty, a syndrome that limits an individual ability to recover from acute stressors. While frailty affects up to 90% of patients with HF with preserved ejection fraction, it is also seen in ~30–60% of patients with HF with reduced ejection fraction, with ~26% higher prevalence in women compared with men. The relationship between frailty and HF is bidirectional, with both conditions exacerbating the other. Frailty is further complicated by a higher prevalence of sarcopenia (by ~20%) in HF patients compared with patients without HF, which negatively affects outcomes. Several frailty assessment methods have been employed historically including the Fried frailty phenotype and Rockwood Clinical Frailty Scale to classify HF patients based on the severity of frailty; however, a validated HF-specific frailty assessment tool does not currently exist. Frailty in HF is associated with a poor prognosis with a 1.5-fold to 2-fold higher risk of all-cause death and hospitalizations compared to non-frail patients. Frailty is also highly prevalent in patients with worsening HF, affecting >50% of patients hospitalized for HF. Such patients with multiple readmissions for decompensated HF have markedly poor outcomes compared to younger, non-frail cohorts, and it is hypothesized that it may be due to major physical and functional limitations that limit recovery from an acute episode of worsening HF, a care aspect that has not been addressed in HF guidelines. Frail patients are thought to confer less benefit from therapeutic interventions due to an increased risk of perceived harm, resulting in lower adherence to HF interventions, which may worsen outcomes. Multiple studies report that <40% of frail patients are on guideline-directed medical therapy for HF, of which most are on suboptimal doses of these medications. There is a lack of evidence generated from randomized trials in this incredibly vulnerable population, and most current practice is governed by post hoc analyses of trials, observational registry-based data and providers' clinical judgement. The current body of evidence suggests that the treatment effect of most guideline-based interventions, including medications, cardiac rehabilitation and device therapy, is consistent across all age groups and frailty subgroups and, in some cases, may be amplified in the older, more frail population. In this review, we discuss the characteristics, assessment tools, impact on prognosis and impact on therapeutic interventions of frailty in patients with HF.</p>","PeriodicalId":186,"journal":{"name":"Journal of Cachexia, Sarcopenia and Muscle","volume":"14 5","pages":"1959-1972"},"PeriodicalIF":9.1000,"publicationDate":"2023-08-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jcsm.13306","citationCount":"1","resultStr":"{\"title\":\"Frailty and heart failure: State-of-the-art review\",\"authors\":\"Khawaja M. Talha, Ambarish Pandey, Marat Fudim, Javed Butler, Stefan D. Anker, Muhammad Shahzeb Khan\",\"doi\":\"10.1002/jcsm.13306\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>At least half of all patients with heart failure (HF) are affected by frailty, a syndrome that limits an individual ability to recover from acute stressors. While frailty affects up to 90% of patients with HF with preserved ejection fraction, it is also seen in ~30–60% of patients with HF with reduced ejection fraction, with ~26% higher prevalence in women compared with men. The relationship between frailty and HF is bidirectional, with both conditions exacerbating the other. Frailty is further complicated by a higher prevalence of sarcopenia (by ~20%) in HF patients compared with patients without HF, which negatively affects outcomes. Several frailty assessment methods have been employed historically including the Fried frailty phenotype and Rockwood Clinical Frailty Scale to classify HF patients based on the severity of frailty; however, a validated HF-specific frailty assessment tool does not currently exist. Frailty in HF is associated with a poor prognosis with a 1.5-fold to 2-fold higher risk of all-cause death and hospitalizations compared to non-frail patients. Frailty is also highly prevalent in patients with worsening HF, affecting >50% of patients hospitalized for HF. Such patients with multiple readmissions for decompensated HF have markedly poor outcomes compared to younger, non-frail cohorts, and it is hypothesized that it may be due to major physical and functional limitations that limit recovery from an acute episode of worsening HF, a care aspect that has not been addressed in HF guidelines. Frail patients are thought to confer less benefit from therapeutic interventions due to an increased risk of perceived harm, resulting in lower adherence to HF interventions, which may worsen outcomes. Multiple studies report that <40% of frail patients are on guideline-directed medical therapy for HF, of which most are on suboptimal doses of these medications. There is a lack of evidence generated from randomized trials in this incredibly vulnerable population, and most current practice is governed by post hoc analyses of trials, observational registry-based data and providers' clinical judgement. The current body of evidence suggests that the treatment effect of most guideline-based interventions, including medications, cardiac rehabilitation and device therapy, is consistent across all age groups and frailty subgroups and, in some cases, may be amplified in the older, more frail population. In this review, we discuss the characteristics, assessment tools, impact on prognosis and impact on therapeutic interventions of frailty in patients with HF.</p>\",\"PeriodicalId\":186,\"journal\":{\"name\":\"Journal of Cachexia, Sarcopenia and Muscle\",\"volume\":\"14 5\",\"pages\":\"1959-1972\"},\"PeriodicalIF\":9.1000,\"publicationDate\":\"2023-08-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jcsm.13306\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cachexia, Sarcopenia and Muscle\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/jcsm.13306\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cachexia, Sarcopenia and Muscle","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jcsm.13306","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Frailty and heart failure: State-of-the-art review
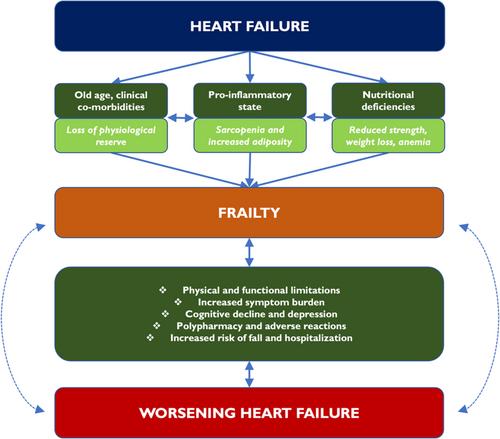
At least half of all patients with heart failure (HF) are affected by frailty, a syndrome that limits an individual ability to recover from acute stressors. While frailty affects up to 90% of patients with HF with preserved ejection fraction, it is also seen in ~30–60% of patients with HF with reduced ejection fraction, with ~26% higher prevalence in women compared with men. The relationship between frailty and HF is bidirectional, with both conditions exacerbating the other. Frailty is further complicated by a higher prevalence of sarcopenia (by ~20%) in HF patients compared with patients without HF, which negatively affects outcomes. Several frailty assessment methods have been employed historically including the Fried frailty phenotype and Rockwood Clinical Frailty Scale to classify HF patients based on the severity of frailty; however, a validated HF-specific frailty assessment tool does not currently exist. Frailty in HF is associated with a poor prognosis with a 1.5-fold to 2-fold higher risk of all-cause death and hospitalizations compared to non-frail patients. Frailty is also highly prevalent in patients with worsening HF, affecting >50% of patients hospitalized for HF. Such patients with multiple readmissions for decompensated HF have markedly poor outcomes compared to younger, non-frail cohorts, and it is hypothesized that it may be due to major physical and functional limitations that limit recovery from an acute episode of worsening HF, a care aspect that has not been addressed in HF guidelines. Frail patients are thought to confer less benefit from therapeutic interventions due to an increased risk of perceived harm, resulting in lower adherence to HF interventions, which may worsen outcomes. Multiple studies report that <40% of frail patients are on guideline-directed medical therapy for HF, of which most are on suboptimal doses of these medications. There is a lack of evidence generated from randomized trials in this incredibly vulnerable population, and most current practice is governed by post hoc analyses of trials, observational registry-based data and providers' clinical judgement. The current body of evidence suggests that the treatment effect of most guideline-based interventions, including medications, cardiac rehabilitation and device therapy, is consistent across all age groups and frailty subgroups and, in some cases, may be amplified in the older, more frail population. In this review, we discuss the characteristics, assessment tools, impact on prognosis and impact on therapeutic interventions of frailty in patients with HF.
期刊介绍:
The Journal of Cachexia, Sarcopenia, and Muscle is a prestigious, peer-reviewed international publication committed to disseminating research and clinical insights pertaining to cachexia, sarcopenia, body composition, and the physiological and pathophysiological alterations occurring throughout the lifespan and in various illnesses across the spectrum of life sciences. This journal serves as a valuable resource for physicians, biochemists, biologists, dieticians, pharmacologists, and students alike.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
