Antonio Coviello, Alessio Bernasconi, Giovanni Balato, Ezio Spasari, Marilena Ianniello, Massimo Mariconda, Maria Vargas, Carmine Iacovazzo, Francesco Smeraglia, Andrea Tognù, Giuseppe Servillo
{"title":"在连续内收管阻滞中,导管尖端在隐神经前方或后方定位:一项单中心回顾性比较研究。","authors":"Antonio Coviello, Alessio Bernasconi, Giovanni Balato, Ezio Spasari, Marilena Ianniello, Massimo Mariconda, Maria Vargas, Carmine Iacovazzo, Francesco Smeraglia, Andrea Tognù, Giuseppe Servillo","doi":"10.2147/LRA.S383601","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and aim: </strong>Ultrasound-guided continuous adductor canal block (cACB) is a conventional choice in patients undergoing total knee arthroplasty (TKA) for the management of the postoperative pain. This study aims to compare different catheter tip locations for cACB relative to the saphenous nerve (anteriorly vs posteriorly) in terms of efficacy and complications.</p><p><strong>Methods: </strong>At the department of Surgical Sciences, Orthopedic Trauma and Emergencies of the University of Naples Federico II (Naples, Italy), between January 2020 and November 2021, retrospective comparative study was executed. Patients planned for TKA were included in the study if they met the follow inclusion criteria: patients undergone TKA; aged 50-85 years; body mass index (BMI) of 18-35 kg/m2; American Society of Anesthesiologists (ASA) physical status classification from I to III; subarachnoid technique for anesthesiology plane; continuous adductor canal block performed by an anesthetist with considerable experience. Patients were assigned to receive cACB with the catheter tip located anteriorly (Group 1, G1) or posteriorly to the saphenous nerve (Group 2, G2). Postoperative pain, ambulation ability, episodes of pump block and rate of catheter dislodgement and leakage were evaluated and analyzed.</p><p><strong>Results: </strong>Altogether, 102 patients were admitted to the study (48 in G1 and 54 in G2). After the first 8 postoperative hours, in G1 17 patients (35.4%) had a VAS greater than 4, while in group 2 only 3 patients (5.6%) had a VAS greater than 4 (p-value <0.01). All patients of both groups showed ambulation ability in the postoperative period. No episode of leakage was recorded. While the catheter displacement rate was similar in the two groups (2.1% for G1 vs 3.7% for G2; p-value >0.05), the episodes of pump block were significantly less in G2 than in G1 (3.7% vs 20.8%; p-value <0.01).</p><p><strong>Conclusion: </strong>In cACB for TKA, we found that positioning the catheter tip posteriorly to the saphenous nerve may lead to a greater postoperative analgesia and reduce the risk of pump block compared to placing the catheter tip anteriorly to the nerve.</p>","PeriodicalId":18203,"journal":{"name":"Local and Regional Anesthesia","volume":"15 ","pages":"97-105"},"PeriodicalIF":1.5000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/30/c9/lra-15-97.PMC9807124.pdf","citationCount":"1","resultStr":"{\"title\":\"Positioning the Catheter Tip Anterior or Posterior to the Saphenous Nerve in Continuous Adductor Canal Block: A Mono-Centric Retrospective Comparative Study.\",\"authors\":\"Antonio Coviello, Alessio Bernasconi, Giovanni Balato, Ezio Spasari, Marilena Ianniello, Massimo Mariconda, Maria Vargas, Carmine Iacovazzo, Francesco Smeraglia, Andrea Tognù, Giuseppe Servillo\",\"doi\":\"10.2147/LRA.S383601\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and aim: </strong>Ultrasound-guided continuous adductor canal block (cACB) is a conventional choice in patients undergoing total knee arthroplasty (TKA) for the management of the postoperative pain. This study aims to compare different catheter tip locations for cACB relative to the saphenous nerve (anteriorly vs posteriorly) in terms of efficacy and complications.</p><p><strong>Methods: </strong>At the department of Surgical Sciences, Orthopedic Trauma and Emergencies of the University of Naples Federico II (Naples, Italy), between January 2020 and November 2021, retrospective comparative study was executed. Patients planned for TKA were included in the study if they met the follow inclusion criteria: patients undergone TKA; aged 50-85 years; body mass index (BMI) of 18-35 kg/m2; American Society of Anesthesiologists (ASA) physical status classification from I to III; subarachnoid technique for anesthesiology plane; continuous adductor canal block performed by an anesthetist with considerable experience. Patients were assigned to receive cACB with the catheter tip located anteriorly (Group 1, G1) or posteriorly to the saphenous nerve (Group 2, G2). Postoperative pain, ambulation ability, episodes of pump block and rate of catheter dislodgement and leakage were evaluated and analyzed.</p><p><strong>Results: </strong>Altogether, 102 patients were admitted to the study (48 in G1 and 54 in G2). After the first 8 postoperative hours, in G1 17 patients (35.4%) had a VAS greater than 4, while in group 2 only 3 patients (5.6%) had a VAS greater than 4 (p-value <0.01). All patients of both groups showed ambulation ability in the postoperative period. No episode of leakage was recorded. While the catheter displacement rate was similar in the two groups (2.1% for G1 vs 3.7% for G2; p-value >0.05), the episodes of pump block were significantly less in G2 than in G1 (3.7% vs 20.8%; p-value <0.01).</p><p><strong>Conclusion: </strong>In cACB for TKA, we found that positioning the catheter tip posteriorly to the saphenous nerve may lead to a greater postoperative analgesia and reduce the risk of pump block compared to placing the catheter tip anteriorly to the nerve.</p>\",\"PeriodicalId\":18203,\"journal\":{\"name\":\"Local and Regional Anesthesia\",\"volume\":\"15 \",\"pages\":\"97-105\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/30/c9/lra-15-97.PMC9807124.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Local and Regional Anesthesia\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/LRA.S383601\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Local and Regional Anesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/LRA.S383601","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 1
摘要
背景与目的:超声引导连续内收管阻滞(cACB)是全膝关节置换术(TKA)患者治疗术后疼痛的常规选择。本研究的目的是比较不同的导管尖端位置相对于隐神经(前部与后部)的疗效和并发症。方法:于2020年1月至2021年11月在意大利那不勒斯费德里科二世大学外科科学、骨科创伤与急诊科进行回顾性比较研究。计划进行TKA的患者如果符合以下纳入标准,则纳入研究:接受TKA的患者;年龄50-85岁;体重指数(BMI) 18-35 kg/m2;美国麻醉医师协会(ASA)身体状态分级从I到III;麻醉平面的蛛网膜下腔技术;由经验丰富的麻醉师进行连续内收管阻滞。患者被分配接受cACB,导管尖端位于隐神经前方(1组,G1)或后方(2组,G2)。评估和分析术后疼痛、行走能力、泵阻塞发生率、导管移位和漏出率。结果:共纳入102例患者(G1 48例,G2 54例)。术后前8 h, G1组有17例(35.4%)患者VAS评分大于4分,而2组只有3例(5.6%)患者VAS评分大于4分(p值0.05),G2组的泵阻发作次数明显少于G1组(3.7% vs 20.8%;结论:在TKA的cACB中,我们发现将导管尖端置于隐神经后方比将导管尖端置于神经前方可获得更大的术后镇痛效果,并降低泵阻塞的风险。
Positioning the Catheter Tip Anterior or Posterior to the Saphenous Nerve in Continuous Adductor Canal Block: A Mono-Centric Retrospective Comparative Study.
Background and aim: Ultrasound-guided continuous adductor canal block (cACB) is a conventional choice in patients undergoing total knee arthroplasty (TKA) for the management of the postoperative pain. This study aims to compare different catheter tip locations for cACB relative to the saphenous nerve (anteriorly vs posteriorly) in terms of efficacy and complications.
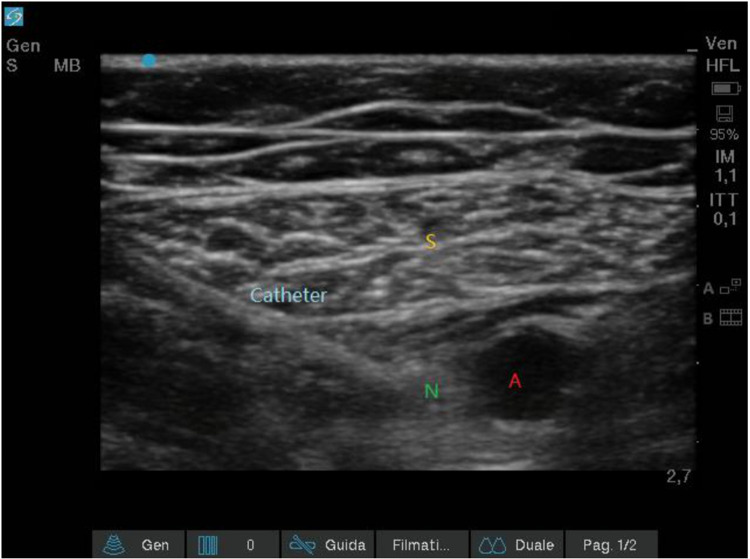
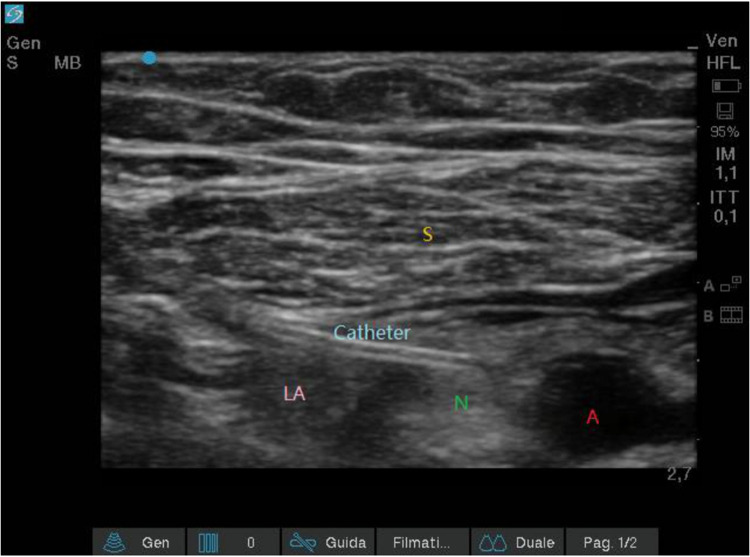
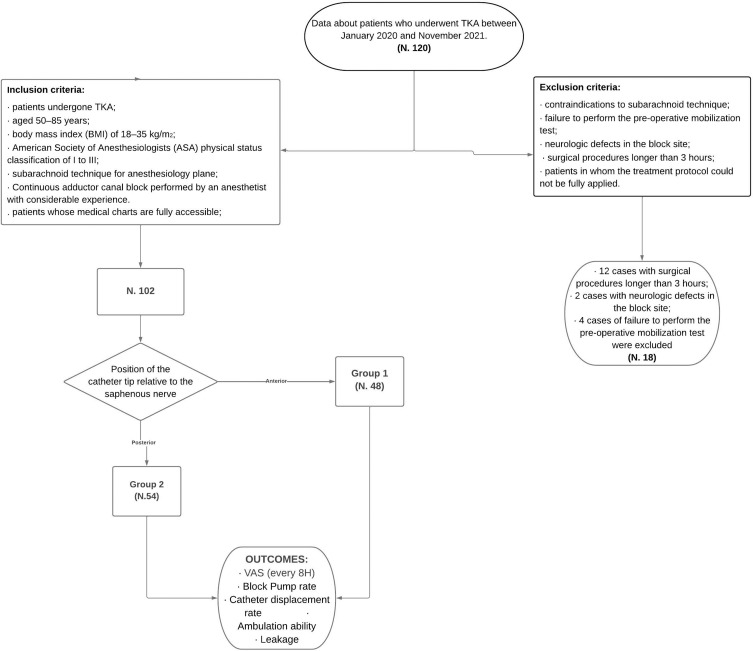
Methods: At the department of Surgical Sciences, Orthopedic Trauma and Emergencies of the University of Naples Federico II (Naples, Italy), between January 2020 and November 2021, retrospective comparative study was executed. Patients planned for TKA were included in the study if they met the follow inclusion criteria: patients undergone TKA; aged 50-85 years; body mass index (BMI) of 18-35 kg/m2; American Society of Anesthesiologists (ASA) physical status classification from I to III; subarachnoid technique for anesthesiology plane; continuous adductor canal block performed by an anesthetist with considerable experience. Patients were assigned to receive cACB with the catheter tip located anteriorly (Group 1, G1) or posteriorly to the saphenous nerve (Group 2, G2). Postoperative pain, ambulation ability, episodes of pump block and rate of catheter dislodgement and leakage were evaluated and analyzed.
Results: Altogether, 102 patients were admitted to the study (48 in G1 and 54 in G2). After the first 8 postoperative hours, in G1 17 patients (35.4%) had a VAS greater than 4, while in group 2 only 3 patients (5.6%) had a VAS greater than 4 (p-value <0.01). All patients of both groups showed ambulation ability in the postoperative period. No episode of leakage was recorded. While the catheter displacement rate was similar in the two groups (2.1% for G1 vs 3.7% for G2; p-value >0.05), the episodes of pump block were significantly less in G2 than in G1 (3.7% vs 20.8%; p-value <0.01).
Conclusion: In cACB for TKA, we found that positioning the catheter tip posteriorly to the saphenous nerve may lead to a greater postoperative analgesia and reduce the risk of pump block compared to placing the catheter tip anteriorly to the nerve.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
