{"title":"早期非小细胞肺癌放射学与病理学肿瘤大小的差异:一项多中心研究。","authors":"Atsushi Kamigaichi MD , Yasuhiro Tsutani MD, PhD , Takahiro Mimae MD, PhD , Yoshihiro Miyata MD, PhD , Hiroyuki Adachi MD, PhD , Yoshihisa Shimada MD, PhD , Yukio Takeshima MD, PhD , Hiroyuki Ito MD, PhD , Norihiko Ikeda MD, PhD , Morihito Okada MD, PhD","doi":"10.1053/j.semtcvs.2022.12.001","DOIUrl":null,"url":null,"abstract":"<div><p><span><span>Discrepancies between radiological whole tumor size (RTS) and pathological whole tumor size (PTS) are sometimes observed. Unexpected pathological upsize may lead to insufficient margins during procedures like sub lobar resections. Therefore, this study aimed to investigate the current status of these discrepancies and identify factors resulting in pathological upsize in patients with early-stage non-small cell lung cancer (NSCLC). Data from a multicenter database of 3092 patients with clinical stage 0-IA NSCLC who underwent </span>pulmonary resection<span> were retrospectively analyzed. Differences between the RTS and PTS were evaluated using Pearson's correlation analysis and Bland-Altman plots. Unexpected pathological upsize was defined as an upsize of ≥1 cm when compared to the RTS, and the predictive factors of this upsize were identified based on multivariable analyses. The RTS and PTS showed a positive linear relationship (</span></span><em>r</em><span> = 0.659), and the RTS slightly overestimated the PTS. The Bland-Altman plot showed 131 of 3092 (5.2%) cases were over the upper 95% limits of agreement. In multivariable analyses, a maximum standardized uptake value (SUV</span><sub>max</sub>) of the primary tumor on 18-fluoro-2-deoxyglucose positron emission tomography/computed tomography (odds ratio [OR], 1.070; 95% confidence interval [CI], 1.035−1.107; <em>P</em> < 0.001) and the adenocarcinoma histology (OR, 1.899; 95% CI, 1.071−3.369; <em>P</em> =0.049) were independent predictors of unexpected pathological upsize. More of the adenocarcinomas with pathological upsize were moderately or poorly differentiated, when compared to those without. The RTS tends to overestimate the PTS; however, care needs to be taken regarding unexpected pathological upsize, especially in adenocarcinomas with a high SUV<sub>max</sub>.</p></div>","PeriodicalId":48592,"journal":{"name":"Seminars in Thoracic and Cardiovascular Surgery","volume":"36 2","pages":"Pages 273-281"},"PeriodicalIF":2.5000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Discrepancy Between Radiological and Pathological Tumor Size in Early-Stage Non-Small Cell Lung Cancer: A Multicenter Study\",\"authors\":\"Atsushi Kamigaichi MD , Yasuhiro Tsutani MD, PhD , Takahiro Mimae MD, PhD , Yoshihiro Miyata MD, PhD , Hiroyuki Adachi MD, PhD , Yoshihisa Shimada MD, PhD , Yukio Takeshima MD, PhD , Hiroyuki Ito MD, PhD , Norihiko Ikeda MD, PhD , Morihito Okada MD, PhD\",\"doi\":\"10.1053/j.semtcvs.2022.12.001\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><p><span><span>Discrepancies between radiological whole tumor size (RTS) and pathological whole tumor size (PTS) are sometimes observed. Unexpected pathological upsize may lead to insufficient margins during procedures like sub lobar resections. Therefore, this study aimed to investigate the current status of these discrepancies and identify factors resulting in pathological upsize in patients with early-stage non-small cell lung cancer (NSCLC). Data from a multicenter database of 3092 patients with clinical stage 0-IA NSCLC who underwent </span>pulmonary resection<span> were retrospectively analyzed. Differences between the RTS and PTS were evaluated using Pearson's correlation analysis and Bland-Altman plots. Unexpected pathological upsize was defined as an upsize of ≥1 cm when compared to the RTS, and the predictive factors of this upsize were identified based on multivariable analyses. The RTS and PTS showed a positive linear relationship (</span></span><em>r</em><span> = 0.659), and the RTS slightly overestimated the PTS. The Bland-Altman plot showed 131 of 3092 (5.2%) cases were over the upper 95% limits of agreement. In multivariable analyses, a maximum standardized uptake value (SUV</span><sub>max</sub>) of the primary tumor on 18-fluoro-2-deoxyglucose positron emission tomography/computed tomography (odds ratio [OR], 1.070; 95% confidence interval [CI], 1.035−1.107; <em>P</em> < 0.001) and the adenocarcinoma histology (OR, 1.899; 95% CI, 1.071−3.369; <em>P</em> =0.049) were independent predictors of unexpected pathological upsize. More of the adenocarcinomas with pathological upsize were moderately or poorly differentiated, when compared to those without. The RTS tends to overestimate the PTS; however, care needs to be taken regarding unexpected pathological upsize, especially in adenocarcinomas with a high SUV<sub>max</sub>.</p></div>\",\"PeriodicalId\":48592,\"journal\":{\"name\":\"Seminars in Thoracic and Cardiovascular Surgery\",\"volume\":\"36 2\",\"pages\":\"Pages 273-281\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2024-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Seminars in Thoracic and Cardiovascular Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S1043067922002775\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/12/10 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Seminars in Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1043067922002775","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/12/10 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Discrepancy Between Radiological and Pathological Tumor Size in Early-Stage Non-Small Cell Lung Cancer: A Multicenter Study
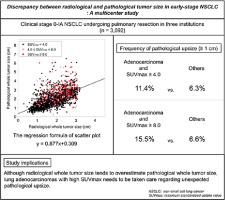
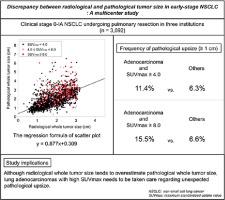
Discrepancies between radiological whole tumor size (RTS) and pathological whole tumor size (PTS) are sometimes observed. Unexpected pathological upsize may lead to insufficient margins during procedures like sub lobar resections. Therefore, this study aimed to investigate the current status of these discrepancies and identify factors resulting in pathological upsize in patients with early-stage non-small cell lung cancer (NSCLC). Data from a multicenter database of 3092 patients with clinical stage 0-IA NSCLC who underwent pulmonary resection were retrospectively analyzed. Differences between the RTS and PTS were evaluated using Pearson's correlation analysis and Bland-Altman plots. Unexpected pathological upsize was defined as an upsize of ≥1 cm when compared to the RTS, and the predictive factors of this upsize were identified based on multivariable analyses. The RTS and PTS showed a positive linear relationship (r = 0.659), and the RTS slightly overestimated the PTS. The Bland-Altman plot showed 131 of 3092 (5.2%) cases were over the upper 95% limits of agreement. In multivariable analyses, a maximum standardized uptake value (SUVmax) of the primary tumor on 18-fluoro-2-deoxyglucose positron emission tomography/computed tomography (odds ratio [OR], 1.070; 95% confidence interval [CI], 1.035−1.107; P < 0.001) and the adenocarcinoma histology (OR, 1.899; 95% CI, 1.071−3.369; P =0.049) were independent predictors of unexpected pathological upsize. More of the adenocarcinomas with pathological upsize were moderately or poorly differentiated, when compared to those without. The RTS tends to overestimate the PTS; however, care needs to be taken regarding unexpected pathological upsize, especially in adenocarcinomas with a high SUVmax.
期刊介绍:
Seminars in Thoracic and Cardiovascular Surgery is devoted to providing a forum for cardiothoracic surgeons to disseminate and discuss important new information and to gain insight into unresolved areas of question in the specialty. Each issue presents readers with a selection of original peer-reviewed articles accompanied by editorial commentary from specialists in the field. In addition, readers are offered valuable invited articles: State of Views editorials and Current Readings highlighting the latest contributions on central or controversial issues. Another prized feature is expert roundtable discussions in which experts debate critical questions for cardiothoracic treatment and care. Seminars is an invitation-only publication that receives original submissions transferred ONLY from its sister publication, The Journal of Thoracic and Cardiovascular Surgery. As we continue to expand the reach of the Journal, we will explore the possibility of accepting unsolicited manuscripts in the future.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
