{"title":"急诊普通外科:预测老年人群的发病率和死亡率。","authors":"Abubaker Elamin, Panagiotis Tsoutsanis, Laith Sinan, Seyedh Paniz Hashemi Tari, Wafa Elamin, Hayato Kurihara","doi":"10.1055/s-0042-1756461","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction</b> Numerous scoring systems have been created to predict the risk of morbidity and mortality in patients undergoing emergency general surgery (EGS). In this article, we compared the different scoring systems utilized at Humanitas Research Hospital and analyzed which one performed the best when assessing geriatric patients (>65 years of age). The scoring systems that were utilized were the APACHE II (Acute Physiology and Chronic Health Evaluation II), ASA (American Society of Anesthesiologists), ACS-NSQIP (American College of Surgeons-National Surgical Quality Improvement Program), Clinical Frailty Score, and the Clavien-Dindo classification as control. <b>Materials and Methods</b> We compiled a database consisting of all patients over the age of 65 who underwent EGS in a consecutive 24-month period between January 1, 2017 and December 31, 2018. We used the biostatistical program \"Stata Version 15\" to analyze our results. <b>Results</b> We found 213 patients who matched our inclusion criteria. Regarding death, we found that the ACS-NSQIP death calculator performed the best with an area under the curve of 0.9017 (odds ratio: 1.09; 95% confidence interval: 1.06-1.12). The APACHE II score had the lowest discriminator when predicting death. Considering short-term complications, the Clavien-Dindo classification scored highly, while both the APACHE II score and Clinical Frailty Score produced the lowest results. <b>Conclusion</b> The results obtained from our research showed that scoring systems and classifications produced different results depending on whether they were used to predict deaths or short-term complications among geriatric patients undergoing EGS.</p>","PeriodicalId":74891,"journal":{"name":"","volume":"8 3","pages":"e270-e278"},"PeriodicalIF":0.0,"publicationDate":"2022-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9512589/pdf/","citationCount":"1","resultStr":"{\"title\":\"Emergency General Surgery: Predicting Morbidity and Mortality in the Geriatric Population.\",\"authors\":\"Abubaker Elamin, Panagiotis Tsoutsanis, Laith Sinan, Seyedh Paniz Hashemi Tari, Wafa Elamin, Hayato Kurihara\",\"doi\":\"10.1055/s-0042-1756461\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Introduction</b> Numerous scoring systems have been created to predict the risk of morbidity and mortality in patients undergoing emergency general surgery (EGS). In this article, we compared the different scoring systems utilized at Humanitas Research Hospital and analyzed which one performed the best when assessing geriatric patients (>65 years of age). The scoring systems that were utilized were the APACHE II (Acute Physiology and Chronic Health Evaluation II), ASA (American Society of Anesthesiologists), ACS-NSQIP (American College of Surgeons-National Surgical Quality Improvement Program), Clinical Frailty Score, and the Clavien-Dindo classification as control. <b>Materials and Methods</b> We compiled a database consisting of all patients over the age of 65 who underwent EGS in a consecutive 24-month period between January 1, 2017 and December 31, 2018. We used the biostatistical program \\\"Stata Version 15\\\" to analyze our results. <b>Results</b> We found 213 patients who matched our inclusion criteria. Regarding death, we found that the ACS-NSQIP death calculator performed the best with an area under the curve of 0.9017 (odds ratio: 1.09; 95% confidence interval: 1.06-1.12). The APACHE II score had the lowest discriminator when predicting death. Considering short-term complications, the Clavien-Dindo classification scored highly, while both the APACHE II score and Clinical Frailty Score produced the lowest results. <b>Conclusion</b> The results obtained from our research showed that scoring systems and classifications produced different results depending on whether they were used to predict deaths or short-term complications among geriatric patients undergoing EGS.</p>\",\"PeriodicalId\":74891,\"journal\":{\"name\":\"\",\"volume\":\"8 3\",\"pages\":\"e270-e278\"},\"PeriodicalIF\":0.0,\"publicationDate\":\"2022-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9512589/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/s-0042-1756461\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0042-1756461","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
摘要
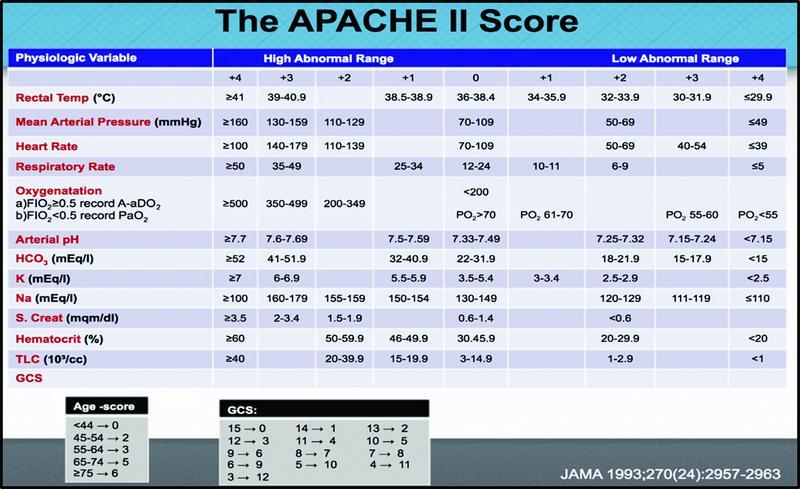
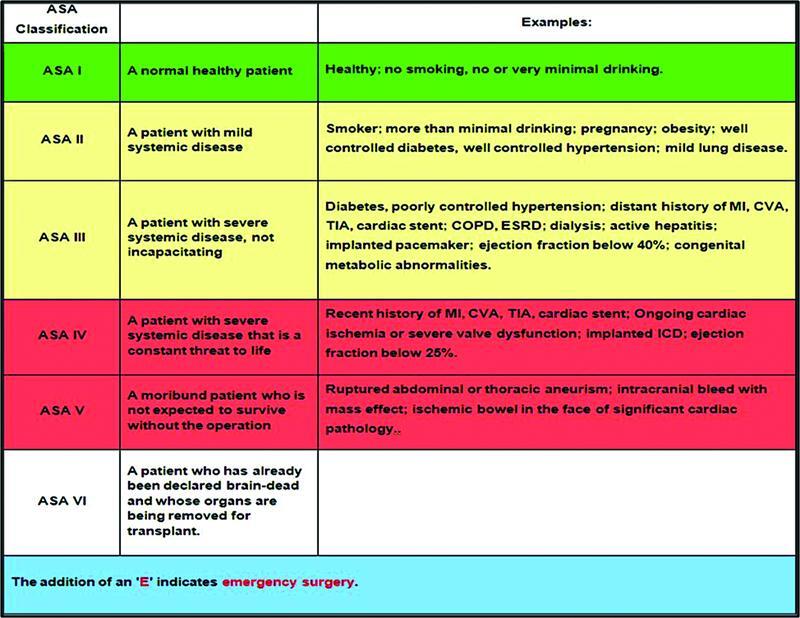
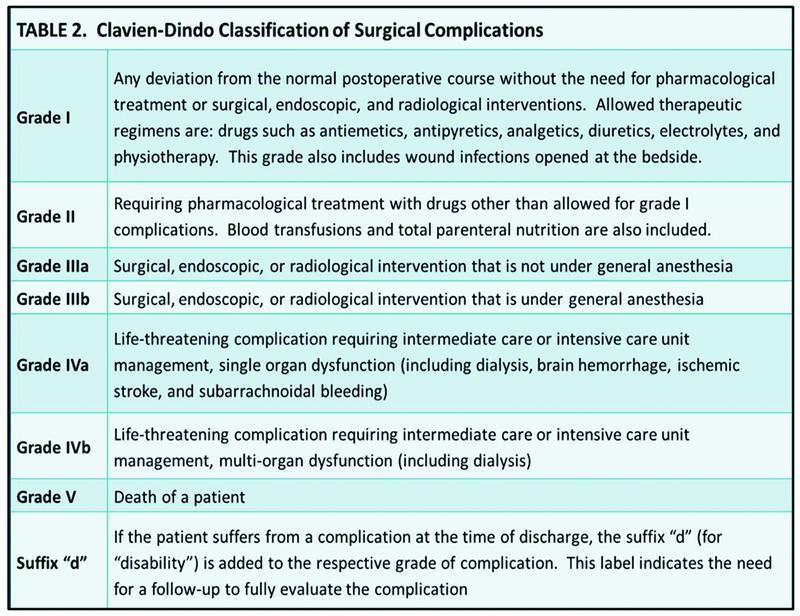
许多评分系统被用来预测急诊普外科(EGS)患者的发病和死亡风险。在本文中,我们比较了Humanitas Research Hospital使用的不同评分系统,并分析了哪一种评分系统在评估老年患者(>65岁)时表现最好。使用的评分系统为APACHE II(急性生理和慢性健康评估II)、ASA(美国麻醉医师学会)、ACS-NSQIP(美国外科医师学会-国家手术质量改进计划)、临床虚弱评分和Clavien-Dindo分类作为对照。材料和方法我们编制了一个数据库,包括2017年1月1日至2018年12月31日连续24个月期间接受EGS治疗的所有65岁以上患者。我们使用生物统计程序“Stata Version 15”来分析我们的结果。结果213例患者符合纳入标准。在死亡方面,我们发现ACS-NSQIP死亡计算器表现最好,曲线下面积为0.9017(优势比:1.09;95%置信区间:1.06-1.12)。APACHE II评分在预测死亡时具有最低的判别性。考虑到短期并发症,Clavien-Dindo评分较高,而APACHE II评分和临床虚弱评分均最低。结论我们的研究结果表明,评分系统和分类是否用于预测老年EGS患者的死亡或短期并发症,会产生不同的结果。
Emergency General Surgery: Predicting Morbidity and Mortality in the Geriatric Population.
Introduction Numerous scoring systems have been created to predict the risk of morbidity and mortality in patients undergoing emergency general surgery (EGS). In this article, we compared the different scoring systems utilized at Humanitas Research Hospital and analyzed which one performed the best when assessing geriatric patients (>65 years of age). The scoring systems that were utilized were the APACHE II (Acute Physiology and Chronic Health Evaluation II), ASA (American Society of Anesthesiologists), ACS-NSQIP (American College of Surgeons-National Surgical Quality Improvement Program), Clinical Frailty Score, and the Clavien-Dindo classification as control. Materials and Methods We compiled a database consisting of all patients over the age of 65 who underwent EGS in a consecutive 24-month period between January 1, 2017 and December 31, 2018. We used the biostatistical program "Stata Version 15" to analyze our results. Results We found 213 patients who matched our inclusion criteria. Regarding death, we found that the ACS-NSQIP death calculator performed the best with an area under the curve of 0.9017 (odds ratio: 1.09; 95% confidence interval: 1.06-1.12). The APACHE II score had the lowest discriminator when predicting death. Considering short-term complications, the Clavien-Dindo classification scored highly, while both the APACHE II score and Clinical Frailty Score produced the lowest results. Conclusion The results obtained from our research showed that scoring systems and classifications produced different results depending on whether they were used to predict deaths or short-term complications among geriatric patients undergoing EGS.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
