Bambang Pujo Semedi, Nancy Margarita Rehatta, Soetjipto Soetjipto, Jusak Nugraha, Muhammad H Mahyuddin, Jannatin N Arnindita, Nabilah A P Wairooy
{"title":"血管紧张素II在降低血管扩张性休克死亡率方面有多有效?系统评价。","authors":"Bambang Pujo Semedi, Nancy Margarita Rehatta, Soetjipto Soetjipto, Jusak Nugraha, Muhammad H Mahyuddin, Jannatin N Arnindita, Nabilah A P Wairooy","doi":"10.2147/OAEM.S391167","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients with severe vasodilation accompanied by refractory hypotension despite high doses of vasopressors were associated with a high mortality rate. The Ang-2 for the Treatment of High-Output Shock (ATHOS) 3 trial demonstrated that angiotensin 2 (Ang-2) could effectively increase MAP and blood pressure in vasodilatory shock patients. This systematic review aims to summarize the impact of Ang-2 for the treatment of vasodilatory shock on clinical outcomes, including length of stay, MAP level (before and after), and mortality also Ang-2 dose needed.</p><p><strong>Methods: </strong>A systematic search in PubMed, Sage, ScienceDirect, Scopus and Gray literature was conducted to obtain studies about the use of Ang-2 in vasodilatory shock patients.</p><p><strong>Results: </strong>In all of the studies that we obtained, there were different results regarding mortality in patients with vasodilatory shock with Ang-2. Mortality was significantly lower when Ang-2 was administered to patients with elevated renin. The initial dose of Ang-2 can be started at 10-20 ng/kg/min, but there is no agreement on the maximum dose. Ang-2 may be considered a third-line vasopressor if the targeted MAP has not been achieved after administration of norepinephrine >200 ng/kg/min for more than 6 hours. Although not statistically significant, the use of Ang-2 can reduce the length of stay in the ICU and in the hospital when compared to patients without Ang-2 therapy, in addition to reducing the dose of vasopressor.</p><p><strong>Conclusion: </strong>Overall, the use of Ang-2 has potential to be a regimen for patients with vasodilatory shock. Further study is needed to obtain more data.</p>","PeriodicalId":74347,"journal":{"name":"","volume":"15 ","pages":"1-11"},"PeriodicalIF":0.0,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/62/5b/oaem-15-1.PMC9830054.pdf","citationCount":"0","resultStr":"{\"title\":\"How Effective is Angiotensin II in Decreasing Mortality of Vasodilatory Shock? A Systematic Review.\",\"authors\":\"Bambang Pujo Semedi, Nancy Margarita Rehatta, Soetjipto Soetjipto, Jusak Nugraha, Muhammad H Mahyuddin, Jannatin N Arnindita, Nabilah A P Wairooy\",\"doi\":\"10.2147/OAEM.S391167\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Patients with severe vasodilation accompanied by refractory hypotension despite high doses of vasopressors were associated with a high mortality rate. The Ang-2 for the Treatment of High-Output Shock (ATHOS) 3 trial demonstrated that angiotensin 2 (Ang-2) could effectively increase MAP and blood pressure in vasodilatory shock patients. This systematic review aims to summarize the impact of Ang-2 for the treatment of vasodilatory shock on clinical outcomes, including length of stay, MAP level (before and after), and mortality also Ang-2 dose needed.</p><p><strong>Methods: </strong>A systematic search in PubMed, Sage, ScienceDirect, Scopus and Gray literature was conducted to obtain studies about the use of Ang-2 in vasodilatory shock patients.</p><p><strong>Results: </strong>In all of the studies that we obtained, there were different results regarding mortality in patients with vasodilatory shock with Ang-2. Mortality was significantly lower when Ang-2 was administered to patients with elevated renin. The initial dose of Ang-2 can be started at 10-20 ng/kg/min, but there is no agreement on the maximum dose. Ang-2 may be considered a third-line vasopressor if the targeted MAP has not been achieved after administration of norepinephrine >200 ng/kg/min for more than 6 hours. Although not statistically significant, the use of Ang-2 can reduce the length of stay in the ICU and in the hospital when compared to patients without Ang-2 therapy, in addition to reducing the dose of vasopressor.</p><p><strong>Conclusion: </strong>Overall, the use of Ang-2 has potential to be a regimen for patients with vasodilatory shock. Further study is needed to obtain more data.</p>\",\"PeriodicalId\":74347,\"journal\":{\"name\":\"\",\"volume\":\"15 \",\"pages\":\"1-11\"},\"PeriodicalIF\":0.0,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/62/5b/oaem-15-1.PMC9830054.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/OAEM.S391167\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/OAEM.S391167","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
How Effective is Angiotensin II in Decreasing Mortality of Vasodilatory Shock? A Systematic Review.
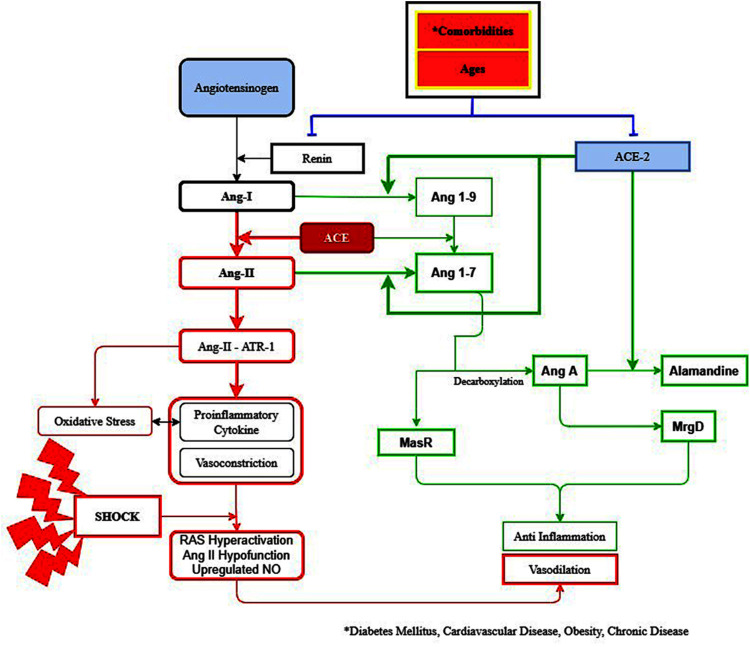
Background: Patients with severe vasodilation accompanied by refractory hypotension despite high doses of vasopressors were associated with a high mortality rate. The Ang-2 for the Treatment of High-Output Shock (ATHOS) 3 trial demonstrated that angiotensin 2 (Ang-2) could effectively increase MAP and blood pressure in vasodilatory shock patients. This systematic review aims to summarize the impact of Ang-2 for the treatment of vasodilatory shock on clinical outcomes, including length of stay, MAP level (before and after), and mortality also Ang-2 dose needed.
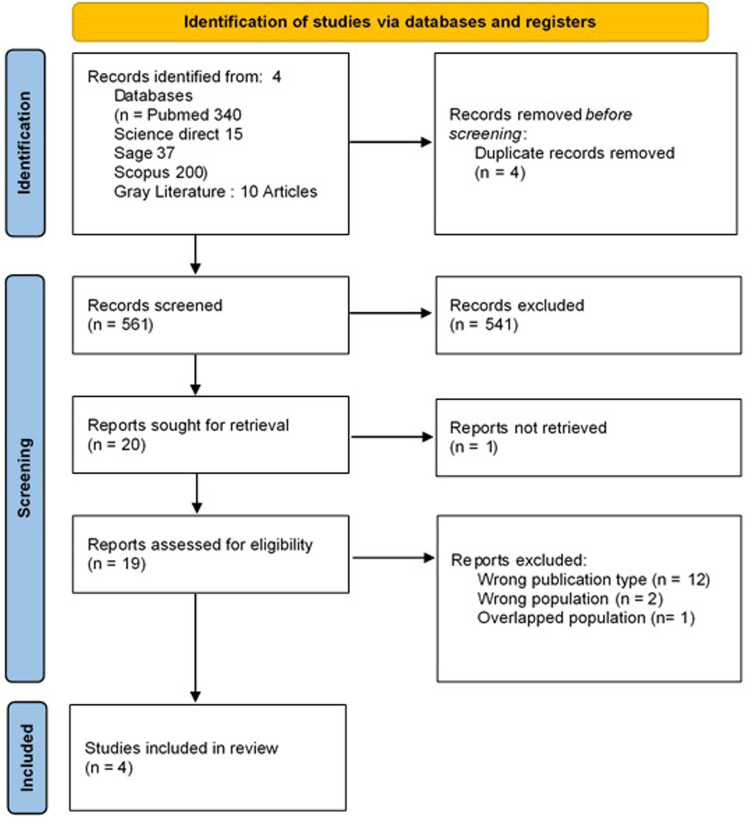
Methods: A systematic search in PubMed, Sage, ScienceDirect, Scopus and Gray literature was conducted to obtain studies about the use of Ang-2 in vasodilatory shock patients.
Results: In all of the studies that we obtained, there were different results regarding mortality in patients with vasodilatory shock with Ang-2. Mortality was significantly lower when Ang-2 was administered to patients with elevated renin. The initial dose of Ang-2 can be started at 10-20 ng/kg/min, but there is no agreement on the maximum dose. Ang-2 may be considered a third-line vasopressor if the targeted MAP has not been achieved after administration of norepinephrine >200 ng/kg/min for more than 6 hours. Although not statistically significant, the use of Ang-2 can reduce the length of stay in the ICU and in the hospital when compared to patients without Ang-2 therapy, in addition to reducing the dose of vasopressor.
Conclusion: Overall, the use of Ang-2 has potential to be a regimen for patients with vasodilatory shock. Further study is needed to obtain more data.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
