Christopher W. Jensen MD MS , Lillian Kang MD , Mary E. Moya-Mendez MS MHS , Kristen E. Rhodin MD MHS , Andrew M. Vekstein MD , W. Schuyler Jones MD , Jennifer A. Rymer MD MBA MHS , Brittany A. Zwischenberger MD , Adam R. Williams MD
{"title":"186例自发性冠状动脉夹层的初步治疗策略和长期疗效。","authors":"Christopher W. Jensen MD MS , Lillian Kang MD , Mary E. Moya-Mendez MS MHS , Kristen E. Rhodin MD MHS , Andrew M. Vekstein MD , W. Schuyler Jones MD , Jennifer A. Rymer MD MBA MHS , Brittany A. Zwischenberger MD , Adam R. Williams MD","doi":"10.1053/j.semtcvs.2023.05.001","DOIUrl":null,"url":null,"abstract":"<div><div><span><span>Spontaneous coronary artery dissection<span> (SCAD) is a rare but important nonatherosclerotic cause of acute coronary syndrome<span><span>. Indications for revascularization<span> and long-term outcomes of SCAD remain areas of active investigation. We report our experience with initial management strategy and long-term outcomes in SCAD. We reviewed all patients treated at our institution from 1996-2021 with a SCAD diagnosis. Demographics, comorbidities, clinical presentations, angiography findings, and management strategies were obtained by chart review. The primary outcome was a composite of cardiac death, recurrent/progressive SCAD, subsequent diagnosis of </span></span>congestive heart failure, or subsequent/repeat revascularization after the initial management. Unadjusted Kaplan-Meier survival analysis was performed. Of 186 patients with a SCAD diagnosis treated at our institution, 149 (80%) were female. Medical management was the initial treatment in 134 (72.0%) patients, percutaneous coronary intervention (PCI) in 43 (23.1%), and </span></span></span>coronary artery bypass grafting in 9 (4.8%). Surgery/PCI intervention was associated with younger age (38.8 vs 47.7 years, </span><em>P</em><span> = 0.01), ST elevation myocardial infarction on presentation (67.0% vs 34.0%, </span><em>P</em><span> < 0.001), lower ejection fraction (45.0% vs 55.0%, </span><em>P</em><span> = 0.002), and left anterior descending coronary artery dissection (75.0% vs 51.0%, </span><em>P</em> = 0.006). Ten-year freedom from our composite outcome was similar between revascularized patients and those managed with medical therapy (<em>P</em><span> = 0.36). Median follow-up time was 4.5 years. SCAD in the setting of ST elevation myocardial infarction, left anterior descending coronary artery involvement, or decreased cardiac function suggests greater ischemic insult and was associated with initial percutaneous or surgical revascularization. Despite worse disease on initial presentation, long-term outcomes of patients undergoing revascularization are similar to medically managed patients with SCAD.</span></div></div>","PeriodicalId":48592,"journal":{"name":"Seminars in Thoracic and Cardiovascular Surgery","volume":"36 4","pages":"Pages 387-397"},"PeriodicalIF":2.5000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Initial Management Strategy and Long-Term Outcomes in 186 Cases of Spontaneous Coronary Artery Dissection\",\"authors\":\"Christopher W. Jensen MD MS , Lillian Kang MD , Mary E. Moya-Mendez MS MHS , Kristen E. Rhodin MD MHS , Andrew M. Vekstein MD , W. Schuyler Jones MD , Jennifer A. Rymer MD MBA MHS , Brittany A. Zwischenberger MD , Adam R. Williams MD\",\"doi\":\"10.1053/j.semtcvs.2023.05.001\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><div><span><span>Spontaneous coronary artery dissection<span> (SCAD) is a rare but important nonatherosclerotic cause of acute coronary syndrome<span><span>. Indications for revascularization<span> and long-term outcomes of SCAD remain areas of active investigation. We report our experience with initial management strategy and long-term outcomes in SCAD. We reviewed all patients treated at our institution from 1996-2021 with a SCAD diagnosis. Demographics, comorbidities, clinical presentations, angiography findings, and management strategies were obtained by chart review. The primary outcome was a composite of cardiac death, recurrent/progressive SCAD, subsequent diagnosis of </span></span>congestive heart failure, or subsequent/repeat revascularization after the initial management. Unadjusted Kaplan-Meier survival analysis was performed. Of 186 patients with a SCAD diagnosis treated at our institution, 149 (80%) were female. Medical management was the initial treatment in 134 (72.0%) patients, percutaneous coronary intervention (PCI) in 43 (23.1%), and </span></span></span>coronary artery bypass grafting in 9 (4.8%). Surgery/PCI intervention was associated with younger age (38.8 vs 47.7 years, </span><em>P</em><span> = 0.01), ST elevation myocardial infarction on presentation (67.0% vs 34.0%, </span><em>P</em><span> < 0.001), lower ejection fraction (45.0% vs 55.0%, </span><em>P</em><span> = 0.002), and left anterior descending coronary artery dissection (75.0% vs 51.0%, </span><em>P</em> = 0.006). Ten-year freedom from our composite outcome was similar between revascularized patients and those managed with medical therapy (<em>P</em><span> = 0.36). Median follow-up time was 4.5 years. SCAD in the setting of ST elevation myocardial infarction, left anterior descending coronary artery involvement, or decreased cardiac function suggests greater ischemic insult and was associated with initial percutaneous or surgical revascularization. Despite worse disease on initial presentation, long-term outcomes of patients undergoing revascularization are similar to medically managed patients with SCAD.</span></div></div>\",\"PeriodicalId\":48592,\"journal\":{\"name\":\"Seminars in Thoracic and Cardiovascular Surgery\",\"volume\":\"36 4\",\"pages\":\"Pages 387-397\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2024-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Seminars in Thoracic and Cardiovascular Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S1043067923000886\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/8/25 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Seminars in Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1043067923000886","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/8/25 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
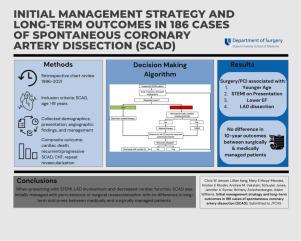
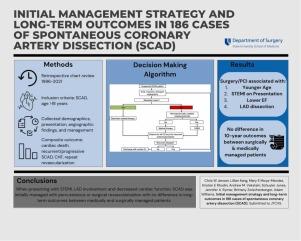
Initial Management Strategy and Long-Term Outcomes in 186 Cases of Spontaneous Coronary Artery Dissection
Spontaneous coronary artery dissection (SCAD) is a rare but important nonatherosclerotic cause of acute coronary syndrome. Indications for revascularization and long-term outcomes of SCAD remain areas of active investigation. We report our experience with initial management strategy and long-term outcomes in SCAD. We reviewed all patients treated at our institution from 1996-2021 with a SCAD diagnosis. Demographics, comorbidities, clinical presentations, angiography findings, and management strategies were obtained by chart review. The primary outcome was a composite of cardiac death, recurrent/progressive SCAD, subsequent diagnosis of congestive heart failure, or subsequent/repeat revascularization after the initial management. Unadjusted Kaplan-Meier survival analysis was performed. Of 186 patients with a SCAD diagnosis treated at our institution, 149 (80%) were female. Medical management was the initial treatment in 134 (72.0%) patients, percutaneous coronary intervention (PCI) in 43 (23.1%), and coronary artery bypass grafting in 9 (4.8%). Surgery/PCI intervention was associated with younger age (38.8 vs 47.7 years, P = 0.01), ST elevation myocardial infarction on presentation (67.0% vs 34.0%, P < 0.001), lower ejection fraction (45.0% vs 55.0%, P = 0.002), and left anterior descending coronary artery dissection (75.0% vs 51.0%, P = 0.006). Ten-year freedom from our composite outcome was similar between revascularized patients and those managed with medical therapy (P = 0.36). Median follow-up time was 4.5 years. SCAD in the setting of ST elevation myocardial infarction, left anterior descending coronary artery involvement, or decreased cardiac function suggests greater ischemic insult and was associated with initial percutaneous or surgical revascularization. Despite worse disease on initial presentation, long-term outcomes of patients undergoing revascularization are similar to medically managed patients with SCAD.
期刊介绍:
Seminars in Thoracic and Cardiovascular Surgery is devoted to providing a forum for cardiothoracic surgeons to disseminate and discuss important new information and to gain insight into unresolved areas of question in the specialty. Each issue presents readers with a selection of original peer-reviewed articles accompanied by editorial commentary from specialists in the field. In addition, readers are offered valuable invited articles: State of Views editorials and Current Readings highlighting the latest contributions on central or controversial issues. Another prized feature is expert roundtable discussions in which experts debate critical questions for cardiothoracic treatment and care. Seminars is an invitation-only publication that receives original submissions transferred ONLY from its sister publication, The Journal of Thoracic and Cardiovascular Surgery. As we continue to expand the reach of the Journal, we will explore the possibility of accepting unsolicited manuscripts in the future.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
