Mary J Yeh, Elizabeth Lydon, Kimberlee Gauvreau, Kathy J Jenkins, David Slater, Lisa Bergersen
{"title":"探讨先天性心导管插入术中手术时间和严重不良事件的风险。","authors":"Mary J Yeh, Elizabeth Lydon, Kimberlee Gauvreau, Kathy J Jenkins, David Slater, Lisa Bergersen","doi":"10.1136/bmjsit-2022-000142","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>While procedure length is considered an important metric for cardiothoracic surgical procedures, the relationship between procedure length and adverse events (AEs) in congenital cardiac catheterizations has little published data available. Furthermore, most existing congenital cardiac catheterization risk prediction models are built on logistic regression models. This study aimed to characterize the relationship between case length and AE occurrence in congenital cardiac catheterization while adjusting for known risk factors and to investigate the potential role of non-linear analysis in risk modeling.</p><p><strong>Design: </strong>Age, case type, and procedure duration were evaluated for relationships with the primary outcome using logistic regression. Non-linearity of the associations with continuous risk factors was assessed using restricted cubic spline transformations.</p><p><strong>Setting and participants: </strong>All diagnostic and interventional congenital cardiac catheterization cases performed at Boston Children's Hospital between January 1, 2014 and October 31, 2019 were analyzed.</p><p><strong>Main outcome measure: </strong>The primary outcome was defined as the occurrence of any clinically significant (level 3/4/5) AE.</p><p><strong>Results: </strong>A total of 7011 catheterization cases met inclusion criteria, with interventional procedures accounting for 68% of cases. Median case duration was 97 min. A multivariable model including age, procedure type, and case duration showed a significant relationship between case duration and AE occurrence (OR 1.07 per 10 min increase, 95% CI 1.06 to 1.09, p<0.001).</p><p><strong>Conclusions: </strong>This study demonstrated the importance of procedure duration as a potential frontier for procedure risk management. Better understanding of the role of procedure duration in cardiac catheterizations may provide opportunities for quality improvement in patient safety and resource planning.</p>","PeriodicalId":33349,"journal":{"name":"BMJ Surgery Interventions Health Technologies","volume":"5 1","pages":"e000142"},"PeriodicalIF":1.6000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ec/e3/bmjsit-2022-000142.PMC9835933.pdf","citationCount":"0","resultStr":"{\"title\":\"Exploring procedure duration and risk for serious adverse events during congenital cardiac catheterization.\",\"authors\":\"Mary J Yeh, Elizabeth Lydon, Kimberlee Gauvreau, Kathy J Jenkins, David Slater, Lisa Bergersen\",\"doi\":\"10.1136/bmjsit-2022-000142\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>While procedure length is considered an important metric for cardiothoracic surgical procedures, the relationship between procedure length and adverse events (AEs) in congenital cardiac catheterizations has little published data available. Furthermore, most existing congenital cardiac catheterization risk prediction models are built on logistic regression models. This study aimed to characterize the relationship between case length and AE occurrence in congenital cardiac catheterization while adjusting for known risk factors and to investigate the potential role of non-linear analysis in risk modeling.</p><p><strong>Design: </strong>Age, case type, and procedure duration were evaluated for relationships with the primary outcome using logistic regression. Non-linearity of the associations with continuous risk factors was assessed using restricted cubic spline transformations.</p><p><strong>Setting and participants: </strong>All diagnostic and interventional congenital cardiac catheterization cases performed at Boston Children's Hospital between January 1, 2014 and October 31, 2019 were analyzed.</p><p><strong>Main outcome measure: </strong>The primary outcome was defined as the occurrence of any clinically significant (level 3/4/5) AE.</p><p><strong>Results: </strong>A total of 7011 catheterization cases met inclusion criteria, with interventional procedures accounting for 68% of cases. Median case duration was 97 min. A multivariable model including age, procedure type, and case duration showed a significant relationship between case duration and AE occurrence (OR 1.07 per 10 min increase, 95% CI 1.06 to 1.09, p<0.001).</p><p><strong>Conclusions: </strong>This study demonstrated the importance of procedure duration as a potential frontier for procedure risk management. Better understanding of the role of procedure duration in cardiac catheterizations may provide opportunities for quality improvement in patient safety and resource planning.</p>\",\"PeriodicalId\":33349,\"journal\":{\"name\":\"BMJ Surgery Interventions Health Technologies\",\"volume\":\"5 1\",\"pages\":\"e000142\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2023-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ec/e3/bmjsit-2022-000142.PMC9835933.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Surgery Interventions Health Technologies\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjsit-2022-000142\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Surgery Interventions Health Technologies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjsit-2022-000142","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
Exploring procedure duration and risk for serious adverse events during congenital cardiac catheterization.
Objectives: While procedure length is considered an important metric for cardiothoracic surgical procedures, the relationship between procedure length and adverse events (AEs) in congenital cardiac catheterizations has little published data available. Furthermore, most existing congenital cardiac catheterization risk prediction models are built on logistic regression models. This study aimed to characterize the relationship between case length and AE occurrence in congenital cardiac catheterization while adjusting for known risk factors and to investigate the potential role of non-linear analysis in risk modeling.
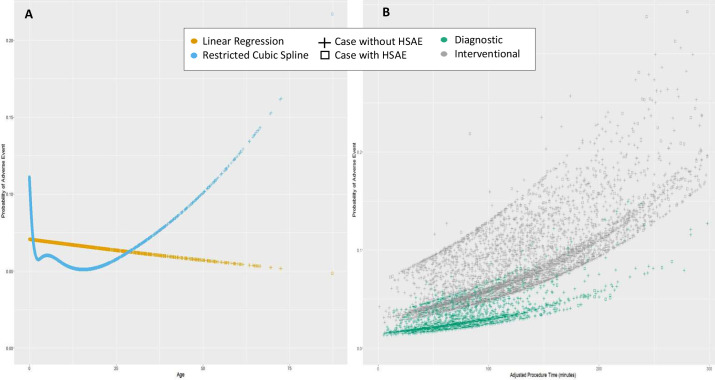
Design: Age, case type, and procedure duration were evaluated for relationships with the primary outcome using logistic regression. Non-linearity of the associations with continuous risk factors was assessed using restricted cubic spline transformations.
Setting and participants: All diagnostic and interventional congenital cardiac catheterization cases performed at Boston Children's Hospital between January 1, 2014 and October 31, 2019 were analyzed.
Main outcome measure: The primary outcome was defined as the occurrence of any clinically significant (level 3/4/5) AE.
Results: A total of 7011 catheterization cases met inclusion criteria, with interventional procedures accounting for 68% of cases. Median case duration was 97 min. A multivariable model including age, procedure type, and case duration showed a significant relationship between case duration and AE occurrence (OR 1.07 per 10 min increase, 95% CI 1.06 to 1.09, p<0.001).
Conclusions: This study demonstrated the importance of procedure duration as a potential frontier for procedure risk management. Better understanding of the role of procedure duration in cardiac catheterizations may provide opportunities for quality improvement in patient safety and resource planning.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
