{"title":"解构ADAURA:是时候放弃IB-IIIA EGFR+ NSCLC的辅助铂基化疗了(除了RB改变?)当采用辅助奥希替尼。","authors":"Shannon S Zhang, Sai-Hong Ignatius Ou","doi":"10.2147/LCTT.S358902","DOIUrl":null,"url":null,"abstract":"<p><p>Adjuvant cisplatin-based chemotherapy is considered the standard of care for resected stage IB (tumor ≥ 4m)-IIIA non-small cell lung cancer (NSCLC). The ADAURA trial is a randomized placebo-controlled Phase III trial that demonstrated statistically significant improved disease-free survival (DFS) with the use of 3-years of adjuvant osimertinib in resected stage IB-IIIA NSCLC harboring epidermal growth factor receptor (<i>EGFR</i>) del 19 or L858R mutations. Subgroup analysis revealed that the DFS improvement with adjuvant osimertinib is independent of adjuvant chemotherapy in the primary analysis. A recent follow-up report suggested that adjuvant cisplatin-based chemotherapy provided no additional 2-year DFS improvement on top of adjuvant osimertinib regardless of stage (IB, II, or IIIA) and minimal numerical DFS benefit in stage II or IIIA resected <i>EGFR+</i> NSCLC for those patients who did not receive adjuvant osimertinib. Here, we argue that if clinicians adopt the use of 3 years of adjuvant osimertinib in resected early-stage <i>EGFR+</i> NSCLC, there is no role for adjuvant platinum-based chemotherapy. The use of adjuvant chemotherapy was balanced between the osimertinib and the placebo arms by stage even though adjuvant chemotherapy was not one of the three stratification factors (del 19 vs L858R; Stage IA vs II vs III; Asians versus non-Asian) in ADAURA. There may be a potential role of adjuvant cisplatin/vinorelbine in a small subgroup of <i>EGFR+</i> NSCLC patients whose tumor harbors retinoblastoma (<i>RB</i>) gene alterations but requires further investigation.</p>","PeriodicalId":74088,"journal":{"name":"","volume":"13 ","pages":"23-31"},"PeriodicalIF":0.0,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6a/a6/lctt-13-23.PMC9057228.pdf","citationCount":"3","resultStr":"{\"title\":\"Deconstructing ADAURA: It is Time to Forgo Adjuvant Platinum-Based Chemotherapy in Resected IB-IIIA <i>EGFR+</i> NSCLC (Except with <i>RB</i> Alterations?) When Adopting Adjuvant Osimertinib.\",\"authors\":\"Shannon S Zhang, Sai-Hong Ignatius Ou\",\"doi\":\"10.2147/LCTT.S358902\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Adjuvant cisplatin-based chemotherapy is considered the standard of care for resected stage IB (tumor ≥ 4m)-IIIA non-small cell lung cancer (NSCLC). The ADAURA trial is a randomized placebo-controlled Phase III trial that demonstrated statistically significant improved disease-free survival (DFS) with the use of 3-years of adjuvant osimertinib in resected stage IB-IIIA NSCLC harboring epidermal growth factor receptor (<i>EGFR</i>) del 19 or L858R mutations. Subgroup analysis revealed that the DFS improvement with adjuvant osimertinib is independent of adjuvant chemotherapy in the primary analysis. A recent follow-up report suggested that adjuvant cisplatin-based chemotherapy provided no additional 2-year DFS improvement on top of adjuvant osimertinib regardless of stage (IB, II, or IIIA) and minimal numerical DFS benefit in stage II or IIIA resected <i>EGFR+</i> NSCLC for those patients who did not receive adjuvant osimertinib. Here, we argue that if clinicians adopt the use of 3 years of adjuvant osimertinib in resected early-stage <i>EGFR+</i> NSCLC, there is no role for adjuvant platinum-based chemotherapy. The use of adjuvant chemotherapy was balanced between the osimertinib and the placebo arms by stage even though adjuvant chemotherapy was not one of the three stratification factors (del 19 vs L858R; Stage IA vs II vs III; Asians versus non-Asian) in ADAURA. There may be a potential role of adjuvant cisplatin/vinorelbine in a small subgroup of <i>EGFR+</i> NSCLC patients whose tumor harbors retinoblastoma (<i>RB</i>) gene alterations but requires further investigation.</p>\",\"PeriodicalId\":74088,\"journal\":{\"name\":\"\",\"volume\":\"13 \",\"pages\":\"23-31\"},\"PeriodicalIF\":0.0,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6a/a6/lctt-13-23.PMC9057228.pdf\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/LCTT.S358902\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/LCTT.S358902","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 3
摘要
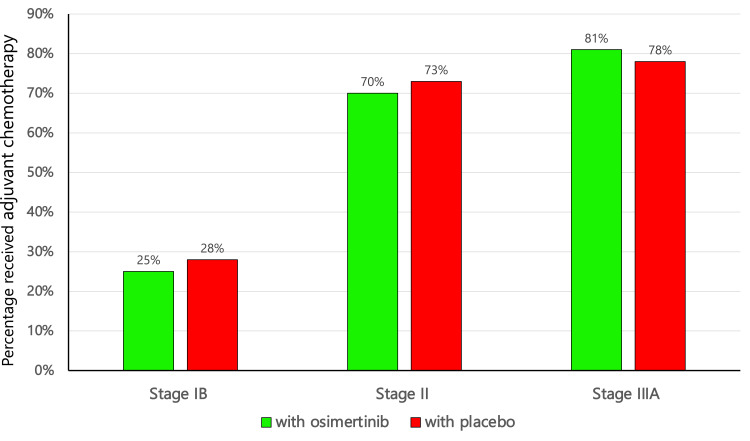
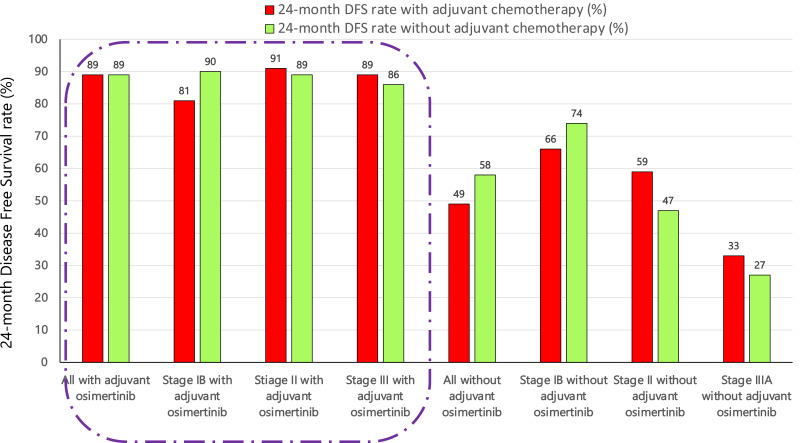
以顺铂为基础的辅助化疗被认为是IB期(肿瘤≥4m)-IIIA期非小细胞肺癌(NSCLC)切除的标准治疗方案。ADAURA试验是一项随机安慰剂对照III期试验,该试验显示,在切除的具有表皮生长因子受体(EGFR) del 19或L858R突变的IB-IIIA期NSCLC中,使用3年辅助奥西替尼可显著提高无病生存率(DFS)。亚组分析显示,在初步分析中,辅助奥希替尼对DFS的改善与辅助化疗无关。最近的一项随访报告表明,在辅助奥西替尼的基础上,辅助顺铂化疗没有提供额外的2年DFS改善,无论分期(IB, II或IIIA),对于那些没有接受辅助奥西替尼的II期或IIIA期EGFR+ NSCLC切除患者,DFS的数值最小。在这里,我们认为,如果临床医生在切除的早期EGFR+ NSCLC中采用3年的辅助奥希替尼,那么基于铂的辅助化疗就没有作用。辅助化疗的使用在奥希替尼组和安慰剂组之间的分期是平衡的,即使辅助化疗不是三个分层因素之一(del 19 vs L858R;IA期vs II期vs III期;亚洲人与非亚洲人)的ADAURA。在一小部分EGFR+ NSCLC患者(其肿瘤含有视网膜母细胞瘤(RB)基因改变)中,顺铂/维诺瑞滨可能具有潜在的辅助作用,但需要进一步研究。
Deconstructing ADAURA: It is Time to Forgo Adjuvant Platinum-Based Chemotherapy in Resected IB-IIIA EGFR+ NSCLC (Except with RB Alterations?) When Adopting Adjuvant Osimertinib.
Adjuvant cisplatin-based chemotherapy is considered the standard of care for resected stage IB (tumor ≥ 4m)-IIIA non-small cell lung cancer (NSCLC). The ADAURA trial is a randomized placebo-controlled Phase III trial that demonstrated statistically significant improved disease-free survival (DFS) with the use of 3-years of adjuvant osimertinib in resected stage IB-IIIA NSCLC harboring epidermal growth factor receptor (EGFR) del 19 or L858R mutations. Subgroup analysis revealed that the DFS improvement with adjuvant osimertinib is independent of adjuvant chemotherapy in the primary analysis. A recent follow-up report suggested that adjuvant cisplatin-based chemotherapy provided no additional 2-year DFS improvement on top of adjuvant osimertinib regardless of stage (IB, II, or IIIA) and minimal numerical DFS benefit in stage II or IIIA resected EGFR+ NSCLC for those patients who did not receive adjuvant osimertinib. Here, we argue that if clinicians adopt the use of 3 years of adjuvant osimertinib in resected early-stage EGFR+ NSCLC, there is no role for adjuvant platinum-based chemotherapy. The use of adjuvant chemotherapy was balanced between the osimertinib and the placebo arms by stage even though adjuvant chemotherapy was not one of the three stratification factors (del 19 vs L858R; Stage IA vs II vs III; Asians versus non-Asian) in ADAURA. There may be a potential role of adjuvant cisplatin/vinorelbine in a small subgroup of EGFR+ NSCLC patients whose tumor harbors retinoblastoma (RB) gene alterations but requires further investigation.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
