{"title":"资源受限的低收入和中等收入国家(LMICS)转移性结直肠癌治疗的情景结局、实践模式和治疗费用评论","authors":"Anant Ramaswamy, Vasu Babu, Rushabh Kothari, Ram Abhinav, Ashwin Desouza, Pradeep Ventrapati, Amit Kumar, Akhil Kapoor, Shasanka Das, Reena Engineer, Avanish Saklani, Vikas Ostwal","doi":"10.1055/s-0041-1736203","DOIUrl":null,"url":null,"abstract":"<p><p>Anant Ramaswamy<b>Introduction</b> The overall survival (OS) of metastatic colorectal cancers (mCRCs) in clinical practice and resource-constrained low- and middle-income countries (LMICS) like India is not known. <b>Materials and Methods</b> Data of patients with mCRC treated between January 2013 and August 2017 were accessed from a prospectively maintained database. Demographics, disease characteristics, chemotherapeutic regimens, use of monoclonal antibodies, and survival outcomes in treated patients were collected and analyzed. Costs of treatment options as off 2017 were also interpreted. <b>Results</b> The data of 403 patients satisfied prespecified inclusion criteria and were included for analysis. The median age of the cohort was 48 years (range: 17-86) with a predominance of rectal cancers (63.3%), liver alone metastases (47.1%), and resected primary (69.7%). Signet ring histology was present in 82 patients (20.3%). The most commonly used first-line regimen (CT1) was modified capecitabine-oxaliplatin (53.3%). Two hundred and nineteen patients (54.3%) received second-line systemic therapy (CT2). Patients received a median of two lines of therapy (range: 1-6). MoAbs were used by 48 patients (13.4%) with CT1 and 34 patients (15.5%) with CT2. Median OS of the entire cohort was 17.61 months (95% confidence interval: 15.48-19.74), which was within the predicted range, as per investigator hypothesis. The presence of signet ring histology ( <i>p</i> <0.001), raised carcinoembryonic antigen at baseline ( <i>p</i> =0.017), and the absence of a resected primary ( <i>p</i> <0.001) predicted inferior median OS. <b>Conclusions</b> Survival of patients with mCRC in a resource-constrained LMIC scenario like India is approximately 12 to 15 months lower than published trial data. Limited access to targeted therapy and newer expensive treatment options due to financial constraints may contribute to this disparity.</p>","PeriodicalId":22053,"journal":{"name":"South Asian Journal of Cancer","volume":"11 4","pages":"293-298"},"PeriodicalIF":0.8000,"publicationDate":"2022-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5d/dc/10-1055-s-0041-1736203.PMC9902092.pdf","citationCount":"0","resultStr":"{\"title\":\"Treatment of Metastatic Colorectal Cancers in Resource-Constrained Low- and Middle-Income Countries (LMICS) Scenario-Outcomes, Practice Patterns, and Commentary on Treatment Costs.\",\"authors\":\"Anant Ramaswamy, Vasu Babu, Rushabh Kothari, Ram Abhinav, Ashwin Desouza, Pradeep Ventrapati, Amit Kumar, Akhil Kapoor, Shasanka Das, Reena Engineer, Avanish Saklani, Vikas Ostwal\",\"doi\":\"10.1055/s-0041-1736203\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Anant Ramaswamy<b>Introduction</b> The overall survival (OS) of metastatic colorectal cancers (mCRCs) in clinical practice and resource-constrained low- and middle-income countries (LMICS) like India is not known. <b>Materials and Methods</b> Data of patients with mCRC treated between January 2013 and August 2017 were accessed from a prospectively maintained database. Demographics, disease characteristics, chemotherapeutic regimens, use of monoclonal antibodies, and survival outcomes in treated patients were collected and analyzed. Costs of treatment options as off 2017 were also interpreted. <b>Results</b> The data of 403 patients satisfied prespecified inclusion criteria and were included for analysis. The median age of the cohort was 48 years (range: 17-86) with a predominance of rectal cancers (63.3%), liver alone metastases (47.1%), and resected primary (69.7%). Signet ring histology was present in 82 patients (20.3%). The most commonly used first-line regimen (CT1) was modified capecitabine-oxaliplatin (53.3%). Two hundred and nineteen patients (54.3%) received second-line systemic therapy (CT2). Patients received a median of two lines of therapy (range: 1-6). MoAbs were used by 48 patients (13.4%) with CT1 and 34 patients (15.5%) with CT2. Median OS of the entire cohort was 17.61 months (95% confidence interval: 15.48-19.74), which was within the predicted range, as per investigator hypothesis. The presence of signet ring histology ( <i>p</i> <0.001), raised carcinoembryonic antigen at baseline ( <i>p</i> =0.017), and the absence of a resected primary ( <i>p</i> <0.001) predicted inferior median OS. <b>Conclusions</b> Survival of patients with mCRC in a resource-constrained LMIC scenario like India is approximately 12 to 15 months lower than published trial data. Limited access to targeted therapy and newer expensive treatment options due to financial constraints may contribute to this disparity.</p>\",\"PeriodicalId\":22053,\"journal\":{\"name\":\"South Asian Journal of Cancer\",\"volume\":\"11 4\",\"pages\":\"293-298\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2022-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/5d/dc/10-1055-s-0041-1736203.PMC9902092.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"South Asian Journal of Cancer\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/s-0041-1736203\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"South Asian Journal of Cancer","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0041-1736203","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
Treatment of Metastatic Colorectal Cancers in Resource-Constrained Low- and Middle-Income Countries (LMICS) Scenario-Outcomes, Practice Patterns, and Commentary on Treatment Costs.
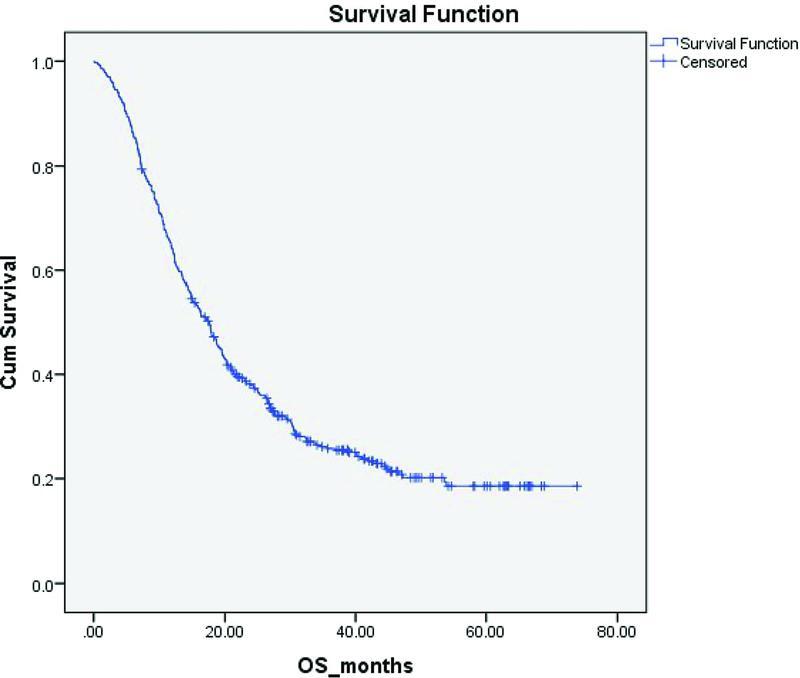
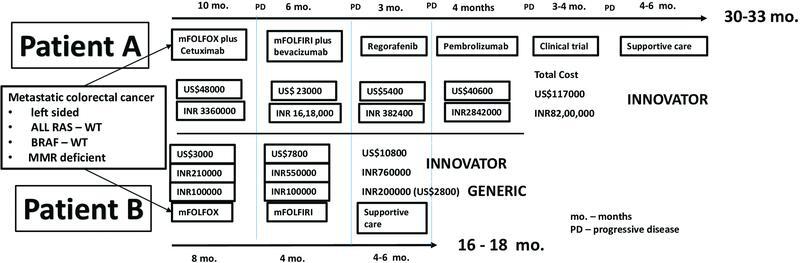
Anant RamaswamyIntroduction The overall survival (OS) of metastatic colorectal cancers (mCRCs) in clinical practice and resource-constrained low- and middle-income countries (LMICS) like India is not known. Materials and Methods Data of patients with mCRC treated between January 2013 and August 2017 were accessed from a prospectively maintained database. Demographics, disease characteristics, chemotherapeutic regimens, use of monoclonal antibodies, and survival outcomes in treated patients were collected and analyzed. Costs of treatment options as off 2017 were also interpreted. Results The data of 403 patients satisfied prespecified inclusion criteria and were included for analysis. The median age of the cohort was 48 years (range: 17-86) with a predominance of rectal cancers (63.3%), liver alone metastases (47.1%), and resected primary (69.7%). Signet ring histology was present in 82 patients (20.3%). The most commonly used first-line regimen (CT1) was modified capecitabine-oxaliplatin (53.3%). Two hundred and nineteen patients (54.3%) received second-line systemic therapy (CT2). Patients received a median of two lines of therapy (range: 1-6). MoAbs were used by 48 patients (13.4%) with CT1 and 34 patients (15.5%) with CT2. Median OS of the entire cohort was 17.61 months (95% confidence interval: 15.48-19.74), which was within the predicted range, as per investigator hypothesis. The presence of signet ring histology ( p <0.001), raised carcinoembryonic antigen at baseline ( p =0.017), and the absence of a resected primary ( p <0.001) predicted inferior median OS. Conclusions Survival of patients with mCRC in a resource-constrained LMIC scenario like India is approximately 12 to 15 months lower than published trial data. Limited access to targeted therapy and newer expensive treatment options due to financial constraints may contribute to this disparity.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
