Carolina Smith, Mikael Hasselgren, Christer Janson, Marta A Kisiel, Karin Lisspers, Anna Nager, Hanna Sandelowsky, Björn Ställberg, Josefin Sundh, Scott Montgomery
{"title":"多病同治是否会导致慢性阻塞性肺病在初级保健中不再优先考虑?","authors":"Carolina Smith, Mikael Hasselgren, Christer Janson, Marta A Kisiel, Karin Lisspers, Anna Nager, Hanna Sandelowsky, Björn Ställberg, Josefin Sundh, Scott Montgomery","doi":"10.1038/s41533-023-00326-x","DOIUrl":null,"url":null,"abstract":"<p><p>The aim of this study was to describe factors associated with having COPD regularly reviewed in primary care by a nurse or physician and assess whether there was de-prioritisation for COPD in multimorbid patients. We defined de-prioritisation as not having at least one check-up by a physician during a two-year period. Among 713 COPD patients in the Swedish PRAXIS study, 473 (66%) had at least one check-up during the study period (ending in 2014). Patients with check-ups were more likely to have three or more comorbid conditions (31.9% vs. 24.6%) and exacerbations (35.1% vs. 21.7%) than those without. Compared with those without comorbidity, those with three or more diagnoses had increased relative risk ratios (and 95% CI) for consultations discussing COPD with only a physician (5.63 (2.68-11.79)), COPD-nurse only (1.67 (0.83-3.37)) or both (2.11 (1.09-4.06)). COPD patients received more frequent check-ups considering COPD if they had comorbidity or a history of exacerbations. We found no evidence of de-prioritisation for COPD in multimorbid patients.</p>","PeriodicalId":19470,"journal":{"name":"NPJ Primary Care Respiratory Medicine","volume":"33 1","pages":"2"},"PeriodicalIF":4.7000,"publicationDate":"2023-01-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9840635/pdf/","citationCount":"0","resultStr":"{\"title\":\"Does multimorbidity result in de-prioritisation of COPD in primary care?\",\"authors\":\"Carolina Smith, Mikael Hasselgren, Christer Janson, Marta A Kisiel, Karin Lisspers, Anna Nager, Hanna Sandelowsky, Björn Ställberg, Josefin Sundh, Scott Montgomery\",\"doi\":\"10.1038/s41533-023-00326-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The aim of this study was to describe factors associated with having COPD regularly reviewed in primary care by a nurse or physician and assess whether there was de-prioritisation for COPD in multimorbid patients. We defined de-prioritisation as not having at least one check-up by a physician during a two-year period. Among 713 COPD patients in the Swedish PRAXIS study, 473 (66%) had at least one check-up during the study period (ending in 2014). Patients with check-ups were more likely to have three or more comorbid conditions (31.9% vs. 24.6%) and exacerbations (35.1% vs. 21.7%) than those without. Compared with those without comorbidity, those with three or more diagnoses had increased relative risk ratios (and 95% CI) for consultations discussing COPD with only a physician (5.63 (2.68-11.79)), COPD-nurse only (1.67 (0.83-3.37)) or both (2.11 (1.09-4.06)). COPD patients received more frequent check-ups considering COPD if they had comorbidity or a history of exacerbations. We found no evidence of de-prioritisation for COPD in multimorbid patients.</p>\",\"PeriodicalId\":19470,\"journal\":{\"name\":\"NPJ Primary Care Respiratory Medicine\",\"volume\":\"33 1\",\"pages\":\"2\"},\"PeriodicalIF\":4.7000,\"publicationDate\":\"2023-01-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9840635/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"NPJ Primary Care Respiratory Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1038/s41533-023-00326-x\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PRIMARY HEALTH CARE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"NPJ Primary Care Respiratory Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1038/s41533-023-00326-x","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PRIMARY HEALTH CARE","Score":null,"Total":0}
Does multimorbidity result in de-prioritisation of COPD in primary care?
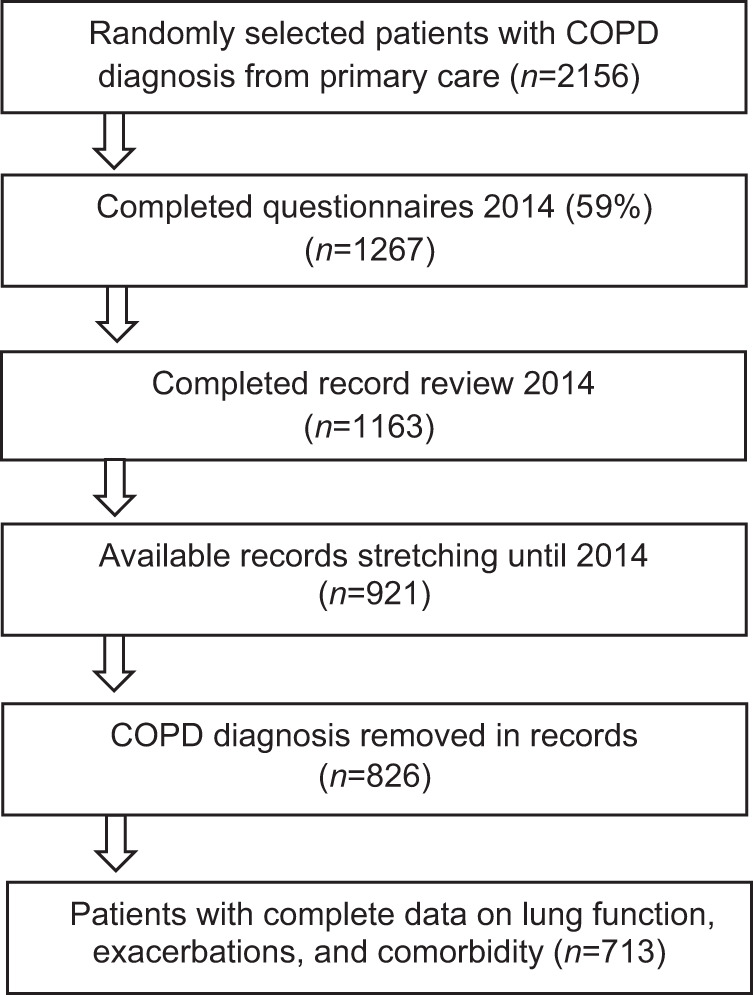
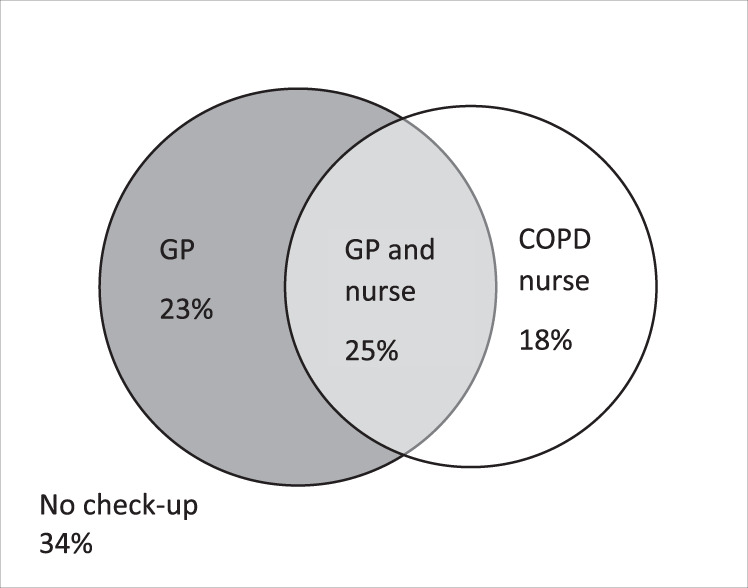
The aim of this study was to describe factors associated with having COPD regularly reviewed in primary care by a nurse or physician and assess whether there was de-prioritisation for COPD in multimorbid patients. We defined de-prioritisation as not having at least one check-up by a physician during a two-year period. Among 713 COPD patients in the Swedish PRAXIS study, 473 (66%) had at least one check-up during the study period (ending in 2014). Patients with check-ups were more likely to have three or more comorbid conditions (31.9% vs. 24.6%) and exacerbations (35.1% vs. 21.7%) than those without. Compared with those without comorbidity, those with three or more diagnoses had increased relative risk ratios (and 95% CI) for consultations discussing COPD with only a physician (5.63 (2.68-11.79)), COPD-nurse only (1.67 (0.83-3.37)) or both (2.11 (1.09-4.06)). COPD patients received more frequent check-ups considering COPD if they had comorbidity or a history of exacerbations. We found no evidence of de-prioritisation for COPD in multimorbid patients.
期刊介绍:
npj Primary Care Respiratory Medicine is an open access, online-only, multidisciplinary journal dedicated to publishing high-quality research in all areas of the primary care management of respiratory and respiratory-related allergic diseases. Papers published by the journal represent important advances of significance to specialists within the fields of primary care and respiratory medicine. We are particularly interested in receiving papers in relation to the following aspects of respiratory medicine, respiratory-related allergic diseases and tobacco control:
epidemiology
prevention
clinical care
service delivery and organisation of healthcare (including implementation science)
global health.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
