Wiebke Solass, Christoph Meisner, Florian Kurtz, Giorgi Nadiradze, Marc A Reymond, Hans Bösmüller
{"title":"腹膜转移的腹膜回归分级评分(PRGS):应该检查多少次活检?","authors":"Wiebke Solass, Christoph Meisner, Florian Kurtz, Giorgi Nadiradze, Marc A Reymond, Hans Bösmüller","doi":"10.1515/pp-2022-0118","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>The four-tied peritoneal regression grading score (PRGS) is increasingly used to evaluate the response of peritoneal metastases (PM) to chemotherapy. The minimal number of peritoneal biopsies needed for PRGS determination remains unclear.</p><p><strong>Methods: </strong>A prospective cohort of 89 PM patients treated with 210 pressurized intraperitoneal aerosol chemotherapy (PIPAC) cycles was investigated. Four biopsies from every abdominal quadrant were recommended. Histological tumor response was defined as a stable or decreasing mean PRGS between therapy cycles, progression increasing. We compared the diagnostic uncertainty induced by missing biopsies to the histological response.</p><p><strong>Results: </strong>A total of 49 patients had at least two PIPAC and were eligible for therapy response assessment. Mean PRGS decreased from 2.04 (CI 5-95% 1.85-2.27) to 1.79 (CI 5-95% 1.59-2.01), p=0.14, as a proof of therapy effectiveness. 35 (71.4%) patients had a stable or decreasing PRGS (therapy response), 14 (28.6%) a PRGS increase (disease progression). Histology showed agreement between four biopsies in 42/210 laparoscopies (20%), between ≥3 biopsies in 103 (49%), and between ≥2 biopsies in 169 laparoscopies (81%). Mean loss of information with one missing biopsy was 0.11 (95% CI=0.13) PRGS points, with two missing biopsies 0.18 (95% CI 0.21). In 9/49 patients (18.3%), the loss of information with one less biopsy exceeded the change in PRGS under therapy.</p><p><strong>Conclusions: </strong>A minimum of three biopsies is needed to diagnose PM progression with an accuracy superior to 80%. Missing biopsies often result in a false diagnosis of tumor progression.</p>","PeriodicalId":20231,"journal":{"name":"Pleura and Peritoneum","volume":"7 4","pages":"179-185"},"PeriodicalIF":2.4000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9742454/pdf/","citationCount":"1","resultStr":"{\"title\":\"Peritoneal regression grading score (PRGS) in peritoneal metastasis: how many biopsies should be examined?\",\"authors\":\"Wiebke Solass, Christoph Meisner, Florian Kurtz, Giorgi Nadiradze, Marc A Reymond, Hans Bösmüller\",\"doi\":\"10.1515/pp-2022-0118\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>The four-tied peritoneal regression grading score (PRGS) is increasingly used to evaluate the response of peritoneal metastases (PM) to chemotherapy. The minimal number of peritoneal biopsies needed for PRGS determination remains unclear.</p><p><strong>Methods: </strong>A prospective cohort of 89 PM patients treated with 210 pressurized intraperitoneal aerosol chemotherapy (PIPAC) cycles was investigated. Four biopsies from every abdominal quadrant were recommended. Histological tumor response was defined as a stable or decreasing mean PRGS between therapy cycles, progression increasing. We compared the diagnostic uncertainty induced by missing biopsies to the histological response.</p><p><strong>Results: </strong>A total of 49 patients had at least two PIPAC and were eligible for therapy response assessment. Mean PRGS decreased from 2.04 (CI 5-95% 1.85-2.27) to 1.79 (CI 5-95% 1.59-2.01), p=0.14, as a proof of therapy effectiveness. 35 (71.4%) patients had a stable or decreasing PRGS (therapy response), 14 (28.6%) a PRGS increase (disease progression). Histology showed agreement between four biopsies in 42/210 laparoscopies (20%), between ≥3 biopsies in 103 (49%), and between ≥2 biopsies in 169 laparoscopies (81%). Mean loss of information with one missing biopsy was 0.11 (95% CI=0.13) PRGS points, with two missing biopsies 0.18 (95% CI 0.21). In 9/49 patients (18.3%), the loss of information with one less biopsy exceeded the change in PRGS under therapy.</p><p><strong>Conclusions: </strong>A minimum of three biopsies is needed to diagnose PM progression with an accuracy superior to 80%. Missing biopsies often result in a false diagnosis of tumor progression.</p>\",\"PeriodicalId\":20231,\"journal\":{\"name\":\"Pleura and Peritoneum\",\"volume\":\"7 4\",\"pages\":\"179-185\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2022-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9742454/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pleura and Peritoneum\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1515/pp-2022-0118\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pleura and Peritoneum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1515/pp-2022-0118","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
Peritoneal regression grading score (PRGS) in peritoneal metastasis: how many biopsies should be examined?
Objectives: The four-tied peritoneal regression grading score (PRGS) is increasingly used to evaluate the response of peritoneal metastases (PM) to chemotherapy. The minimal number of peritoneal biopsies needed for PRGS determination remains unclear.
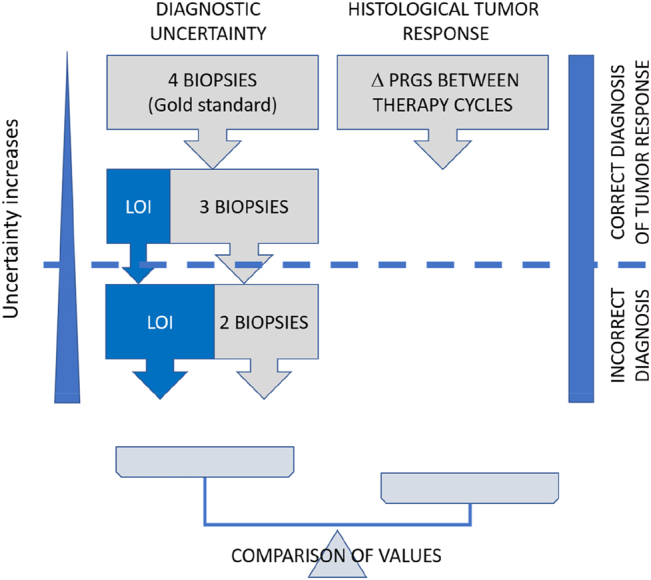
Methods: A prospective cohort of 89 PM patients treated with 210 pressurized intraperitoneal aerosol chemotherapy (PIPAC) cycles was investigated. Four biopsies from every abdominal quadrant were recommended. Histological tumor response was defined as a stable or decreasing mean PRGS between therapy cycles, progression increasing. We compared the diagnostic uncertainty induced by missing biopsies to the histological response.
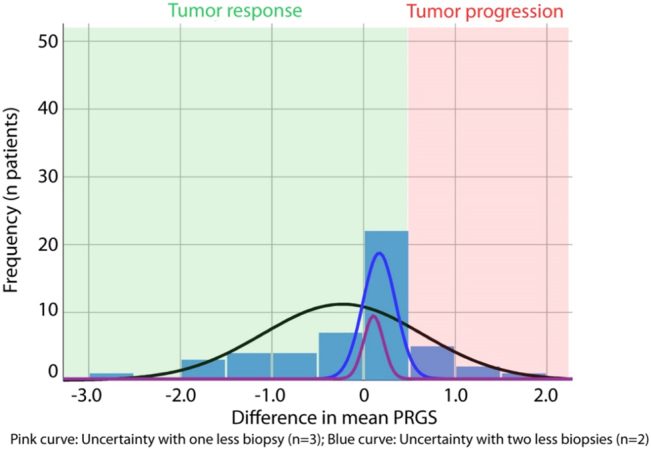
Results: A total of 49 patients had at least two PIPAC and were eligible for therapy response assessment. Mean PRGS decreased from 2.04 (CI 5-95% 1.85-2.27) to 1.79 (CI 5-95% 1.59-2.01), p=0.14, as a proof of therapy effectiveness. 35 (71.4%) patients had a stable or decreasing PRGS (therapy response), 14 (28.6%) a PRGS increase (disease progression). Histology showed agreement between four biopsies in 42/210 laparoscopies (20%), between ≥3 biopsies in 103 (49%), and between ≥2 biopsies in 169 laparoscopies (81%). Mean loss of information with one missing biopsy was 0.11 (95% CI=0.13) PRGS points, with two missing biopsies 0.18 (95% CI 0.21). In 9/49 patients (18.3%), the loss of information with one less biopsy exceeded the change in PRGS under therapy.
Conclusions: A minimum of three biopsies is needed to diagnose PM progression with an accuracy superior to 80%. Missing biopsies often result in a false diagnosis of tumor progression.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
