Jody Ede, David Garry, Graham Barker, Owen Gustafson, Elizabeth King, Hannah Routley, Christopher Biggs, Cherry Lumley, Lyn Bennett, Stephanie Payne, Andrew Ellis, Clinton Green, Nathan Smith, Laura Vincent, Matthew Holdaway, Peter Watkinson
{"title":"构建Covid-19安全重症监护室:以人为本的设计方法。","authors":"Jody Ede, David Garry, Graham Barker, Owen Gustafson, Elizabeth King, Hannah Routley, Christopher Biggs, Cherry Lumley, Lyn Bennett, Stephanie Payne, Andrew Ellis, Clinton Green, Nathan Smith, Laura Vincent, Matthew Holdaway, Peter Watkinson","doi":"10.1177/17511437221092685","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The Covid-19 pandemic has highlighted weaknesses in the National Health Service critical care provision including both capacity and infrastructure. Traditionally, healthcare workspaces have failed to fully incorporate Human-Centred Design principles resulting in environments that negatively affect the efficacy of task completion, patient safety and staff wellbeing. In the summer of 2020, we received funds for the urgent construction of a Covid-19 secure critical care facility. The aim of this project was to design a pandemic resilient facility centred around both staff and patient requirements and safety, within the available footprint.</p><p><strong>Methods: </strong>We developed a simulation exercise, underpinned by Human-Centred Design principles, to evaluate intensive care designs through Build Mapping, Tasks Analysis and Qualitative data. Build Mapping involved taping out sections of the design and mocking up with equipment. Task Analysis and qualitative data were collected following task completion.</p><p><strong>Results: </strong>56 participants completed the build simulation exercise generating 141 design suggestions (69 task related, 56 patient and relative related, 16 staff related). Suggestions translated to 18 multilevel design improvements; five significant structural changes (Macro level) including wall moves and lift size change. Minor improvements were made at a Meso and Micro design level. Critical care design drivers identified included functional drivers (visibility, Covid-19 secure environment, workflow, and task efficiency) and behavioural drivers (learning and development, light, humanising intensive care and design consistency).</p><p><strong>Conclusion: </strong>Success of clinical tasks, infection control, patient safety and staff/patient wellbeing are highly dependent on clinical environments. Primarily, we have improved clinical design by focusing on user requirements. Secondly, we developed a replicable approach to exploring healthcare build plans revealing significant design changes, that may have only been identified once built.</p>","PeriodicalId":39161,"journal":{"name":"Journal of the Intensive Care Society","volume":"24 1","pages":"71-77"},"PeriodicalIF":1.4000,"publicationDate":"2023-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9204129/pdf/","citationCount":"0","resultStr":"{\"title\":\"Building a Covid-19 secure intensive care unit: A human-centred design approach.\",\"authors\":\"Jody Ede, David Garry, Graham Barker, Owen Gustafson, Elizabeth King, Hannah Routley, Christopher Biggs, Cherry Lumley, Lyn Bennett, Stephanie Payne, Andrew Ellis, Clinton Green, Nathan Smith, Laura Vincent, Matthew Holdaway, Peter Watkinson\",\"doi\":\"10.1177/17511437221092685\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The Covid-19 pandemic has highlighted weaknesses in the National Health Service critical care provision including both capacity and infrastructure. Traditionally, healthcare workspaces have failed to fully incorporate Human-Centred Design principles resulting in environments that negatively affect the efficacy of task completion, patient safety and staff wellbeing. In the summer of 2020, we received funds for the urgent construction of a Covid-19 secure critical care facility. The aim of this project was to design a pandemic resilient facility centred around both staff and patient requirements and safety, within the available footprint.</p><p><strong>Methods: </strong>We developed a simulation exercise, underpinned by Human-Centred Design principles, to evaluate intensive care designs through Build Mapping, Tasks Analysis and Qualitative data. Build Mapping involved taping out sections of the design and mocking up with equipment. Task Analysis and qualitative data were collected following task completion.</p><p><strong>Results: </strong>56 participants completed the build simulation exercise generating 141 design suggestions (69 task related, 56 patient and relative related, 16 staff related). Suggestions translated to 18 multilevel design improvements; five significant structural changes (Macro level) including wall moves and lift size change. Minor improvements were made at a Meso and Micro design level. Critical care design drivers identified included functional drivers (visibility, Covid-19 secure environment, workflow, and task efficiency) and behavioural drivers (learning and development, light, humanising intensive care and design consistency).</p><p><strong>Conclusion: </strong>Success of clinical tasks, infection control, patient safety and staff/patient wellbeing are highly dependent on clinical environments. Primarily, we have improved clinical design by focusing on user requirements. Secondly, we developed a replicable approach to exploring healthcare build plans revealing significant design changes, that may have only been identified once built.</p>\",\"PeriodicalId\":39161,\"journal\":{\"name\":\"Journal of the Intensive Care Society\",\"volume\":\"24 1\",\"pages\":\"71-77\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2023-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9204129/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of the Intensive Care Society\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/17511437221092685\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/6/15 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Intensive Care Society","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/17511437221092685","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/6/15 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
Building a Covid-19 secure intensive care unit: A human-centred design approach.
Background: The Covid-19 pandemic has highlighted weaknesses in the National Health Service critical care provision including both capacity and infrastructure. Traditionally, healthcare workspaces have failed to fully incorporate Human-Centred Design principles resulting in environments that negatively affect the efficacy of task completion, patient safety and staff wellbeing. In the summer of 2020, we received funds for the urgent construction of a Covid-19 secure critical care facility. The aim of this project was to design a pandemic resilient facility centred around both staff and patient requirements and safety, within the available footprint.
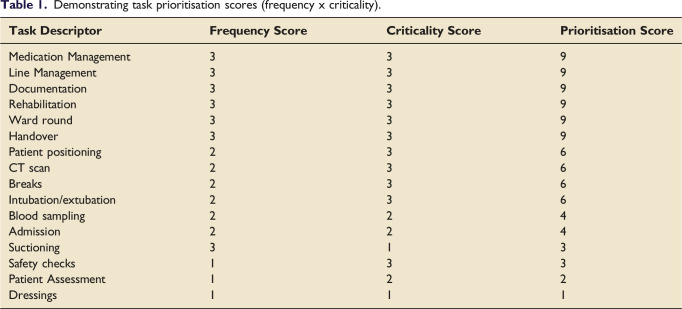
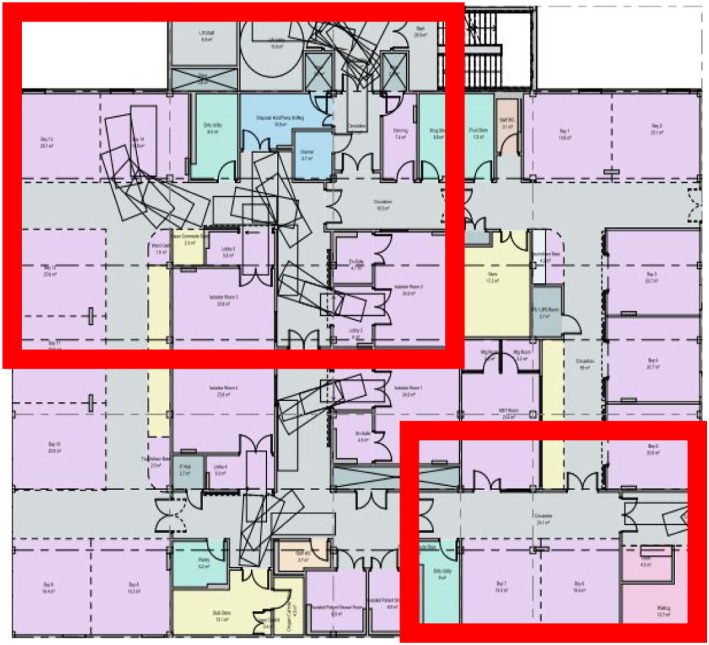
Methods: We developed a simulation exercise, underpinned by Human-Centred Design principles, to evaluate intensive care designs through Build Mapping, Tasks Analysis and Qualitative data. Build Mapping involved taping out sections of the design and mocking up with equipment. Task Analysis and qualitative data were collected following task completion.
Results: 56 participants completed the build simulation exercise generating 141 design suggestions (69 task related, 56 patient and relative related, 16 staff related). Suggestions translated to 18 multilevel design improvements; five significant structural changes (Macro level) including wall moves and lift size change. Minor improvements were made at a Meso and Micro design level. Critical care design drivers identified included functional drivers (visibility, Covid-19 secure environment, workflow, and task efficiency) and behavioural drivers (learning and development, light, humanising intensive care and design consistency).
Conclusion: Success of clinical tasks, infection control, patient safety and staff/patient wellbeing are highly dependent on clinical environments. Primarily, we have improved clinical design by focusing on user requirements. Secondly, we developed a replicable approach to exploring healthcare build plans revealing significant design changes, that may have only been identified once built.
期刊介绍:
The Journal of the Intensive Care Society (JICS) is an international, peer-reviewed journal that strives to disseminate clinically and scientifically relevant peer-reviewed research, evaluation, experience and opinion to all staff working in the field of intensive care medicine. Our aim is to inform clinicians on the provision of best practice and provide direction for innovative scientific research in what is one of the broadest and most multi-disciplinary healthcare specialties. While original articles and systematic reviews lie at the heart of the Journal, we also value and recognise the need for opinion articles, case reports and correspondence to guide clinically and scientifically important areas in which conclusive evidence is lacking. The style of the Journal is based on its founding mission statement to ‘instruct, inform and entertain by encompassing the best aspects of both tabloid and broadsheet''.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
