Per M Arvidsson, Peregrine G Green, William D Watson, Mayooran Shanmuganathan, Einar Heiberg, Giovanni Luigi De Maria, Håkan Arheden, Neil Herring, Oliver J Rider
{"title":"无创左心室压力-容积环心血管磁共振成像和肱血压:使用压力导管测量验证。","authors":"Per M Arvidsson, Peregrine G Green, William D Watson, Mayooran Shanmuganathan, Einar Heiberg, Giovanni Luigi De Maria, Håkan Arheden, Neil Herring, Oliver J Rider","doi":"10.1093/ehjimp/qyad035","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Left ventricular (LV) pressure-volume (PV) loops provide gold-standard physiological information but require invasive measurements of ventricular intracavity pressure, limiting clinical and research applications. A non-invasive method for the computation of PV loops from magnetic resonance imaging and brachial cuff blood pressure has recently been proposed. Here we evaluated the fidelity of the non-invasive PV algorithm against invasive LV pressures in humans.</p><p><strong>Methods and results: </strong>Four heart failure patients with EF < 35% and LV dyssynchrony underwent cardiovascular magnetic resonance (CMR) imaging and subsequent LV catheterization with sequential administration of two different intravenous metabolic substrate infusions (insulin/dextrose and lipid emulsion), producing eight datasets at different haemodynamic states. Pressure-volume loops were computed from CMR volumes combined with (i) a time-varying elastance function scaled to brachial blood pressure and temporally stretched to match volume data, or (ii) invasive pressures averaged from 19 to 30 sampled beats. Method comparison was conducted using linear regression and Bland-Altman analysis. Non-invasively derived PV loop parameters demonstrated high correlation and low bias when compared to invasive data for stroke work (R<sup>2</sup> = 0.96, <i>P</i> < 0.0001, bias 4.6%), potential energy (R<sup>2</sup> = 0.83, <i>P</i> = 0.001, bias 1.5%), end-systolic pressure-volume relationship (R<sup>2</sup> = 0.89, <i>P</i> = 0.0004, bias 5.8%), ventricular efficiency (R<sup>2</sup> = 0.98, <i>P</i> < 0.0001, bias 0.8%), arterial elastance (R<sup>2</sup> = 0.88, <i>P</i> = 0.0006, bias -8.0%), mean external power (R<sup>2</sup> = 0.92, <i>P</i> = 0.0002, bias 4.4%), and energy per ejected volume (R<sup>2</sup> = 0.89, <i>P</i> = 0.0001, bias 3.7%). Variations in estimated end-diastolic pressure did not significantly affect results (<i>P</i> > 0.05 for all). Intraobserver analysis after one year demonstrated 0.9-3.4% bias for LV volumetry and 0.2-5.4% for PV loop-derived parameters.</p><p><strong>Conclusion: </strong>Pressure-volume loops can be precisely and accurately computed from CMR imaging and brachial cuff blood pressure in humans.</p>","PeriodicalId":94317,"journal":{"name":"European heart journal. Imaging methods and practice","volume":"1 2","pages":"qyad035"},"PeriodicalIF":0.0000,"publicationDate":"2023-10-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10631830/pdf/","citationCount":"0","resultStr":"{\"title\":\"Non-invasive left ventricular pressure-volume loops from cardiovascular magnetic resonance imaging and brachial blood pressure: validation using pressure catheter measurements.\",\"authors\":\"Per M Arvidsson, Peregrine G Green, William D Watson, Mayooran Shanmuganathan, Einar Heiberg, Giovanni Luigi De Maria, Håkan Arheden, Neil Herring, Oliver J Rider\",\"doi\":\"10.1093/ehjimp/qyad035\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>Left ventricular (LV) pressure-volume (PV) loops provide gold-standard physiological information but require invasive measurements of ventricular intracavity pressure, limiting clinical and research applications. A non-invasive method for the computation of PV loops from magnetic resonance imaging and brachial cuff blood pressure has recently been proposed. Here we evaluated the fidelity of the non-invasive PV algorithm against invasive LV pressures in humans.</p><p><strong>Methods and results: </strong>Four heart failure patients with EF < 35% and LV dyssynchrony underwent cardiovascular magnetic resonance (CMR) imaging and subsequent LV catheterization with sequential administration of two different intravenous metabolic substrate infusions (insulin/dextrose and lipid emulsion), producing eight datasets at different haemodynamic states. Pressure-volume loops were computed from CMR volumes combined with (i) a time-varying elastance function scaled to brachial blood pressure and temporally stretched to match volume data, or (ii) invasive pressures averaged from 19 to 30 sampled beats. Method comparison was conducted using linear regression and Bland-Altman analysis. Non-invasively derived PV loop parameters demonstrated high correlation and low bias when compared to invasive data for stroke work (R<sup>2</sup> = 0.96, <i>P</i> < 0.0001, bias 4.6%), potential energy (R<sup>2</sup> = 0.83, <i>P</i> = 0.001, bias 1.5%), end-systolic pressure-volume relationship (R<sup>2</sup> = 0.89, <i>P</i> = 0.0004, bias 5.8%), ventricular efficiency (R<sup>2</sup> = 0.98, <i>P</i> < 0.0001, bias 0.8%), arterial elastance (R<sup>2</sup> = 0.88, <i>P</i> = 0.0006, bias -8.0%), mean external power (R<sup>2</sup> = 0.92, <i>P</i> = 0.0002, bias 4.4%), and energy per ejected volume (R<sup>2</sup> = 0.89, <i>P</i> = 0.0001, bias 3.7%). Variations in estimated end-diastolic pressure did not significantly affect results (<i>P</i> > 0.05 for all). Intraobserver analysis after one year demonstrated 0.9-3.4% bias for LV volumetry and 0.2-5.4% for PV loop-derived parameters.</p><p><strong>Conclusion: </strong>Pressure-volume loops can be precisely and accurately computed from CMR imaging and brachial cuff blood pressure in humans.</p>\",\"PeriodicalId\":94317,\"journal\":{\"name\":\"European heart journal. Imaging methods and practice\",\"volume\":\"1 2\",\"pages\":\"qyad035\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-10-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10631830/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal. Imaging methods and practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjimp/qyad035\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Imaging methods and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjimp/qyad035","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
目的:左心室(LV)压力-容积(PV)环路提供了金标准的生理信息,但需要侵入性测量心室腔内压力,限制了临床和研究应用。最近提出了一种从磁共振成像和臂袖血压计算PV环的无创方法。在这里,我们评估了非侵入性PV算法对人类侵入性左室压力的保真度。方法和结果:4例EF < 35%且左室不同步的心力衰竭患者行心血管磁共振(CMR)成像,随后行左室导管置管,并顺序给予两种不同的静脉代谢底物输注(胰岛素/葡萄糖和脂质乳),产生不同血流动力学状态的8个数据集。根据CMR容积计算压力-容积循环,并结合(i)按肱血压缩放的时变弹性函数,并暂时拉伸以匹配容积数据,或(ii) 19至30次采样心跳的平均侵入性压力。方法采用线性回归和Bland-Altman分析进行比较。方法推导出光伏循环参数表现出高度的相关性和低偏差相比,中风的入侵数据工作(R2 = 0.96, P < 0.0001,偏差4.6%),势能(R2 = 0.83, P = 0.001,偏差1.5%),收缩末期压力-容积关系(R2 = 0.89, P = 0.0004,偏差5.8%)、心室效率(R2 = 0.98, P < 0.0001,偏差0.8%),动脉倒电容(R2 = 0.88, P = 0.0006,偏差-8.0%),意思是外部力量(R2 = 0.92, P = 0.0002,偏差4.4%),和每喷射体积能量(R2 = 0.89, P = 0.0001,偏差3.7%)。估计舒张末期压的变化对结果没有显著影响(P < 0.05)。一年后的观察者内部分析显示,左室容积法的偏差为0.9-3.4%,PV环路衍生参数的偏差为0.2-5.4%。结论:通过CMR成像和肱袖带血压可以精确计算出压力-容积环。
Non-invasive left ventricular pressure-volume loops from cardiovascular magnetic resonance imaging and brachial blood pressure: validation using pressure catheter measurements.
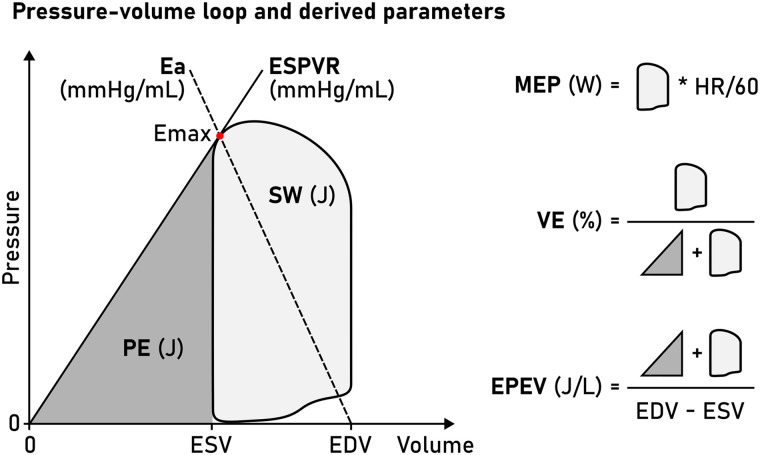
Aims: Left ventricular (LV) pressure-volume (PV) loops provide gold-standard physiological information but require invasive measurements of ventricular intracavity pressure, limiting clinical and research applications. A non-invasive method for the computation of PV loops from magnetic resonance imaging and brachial cuff blood pressure has recently been proposed. Here we evaluated the fidelity of the non-invasive PV algorithm against invasive LV pressures in humans.
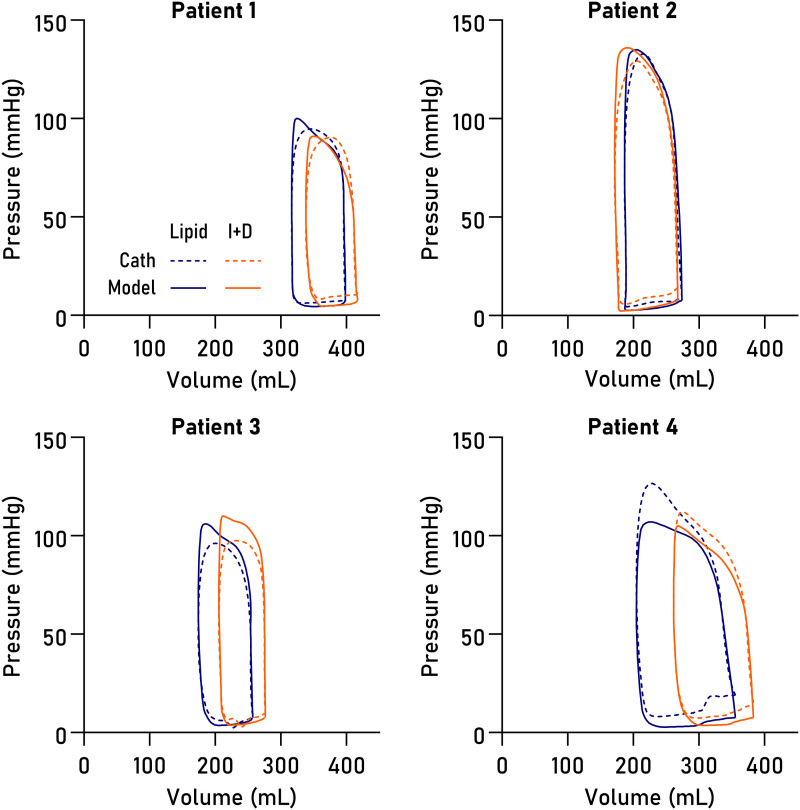
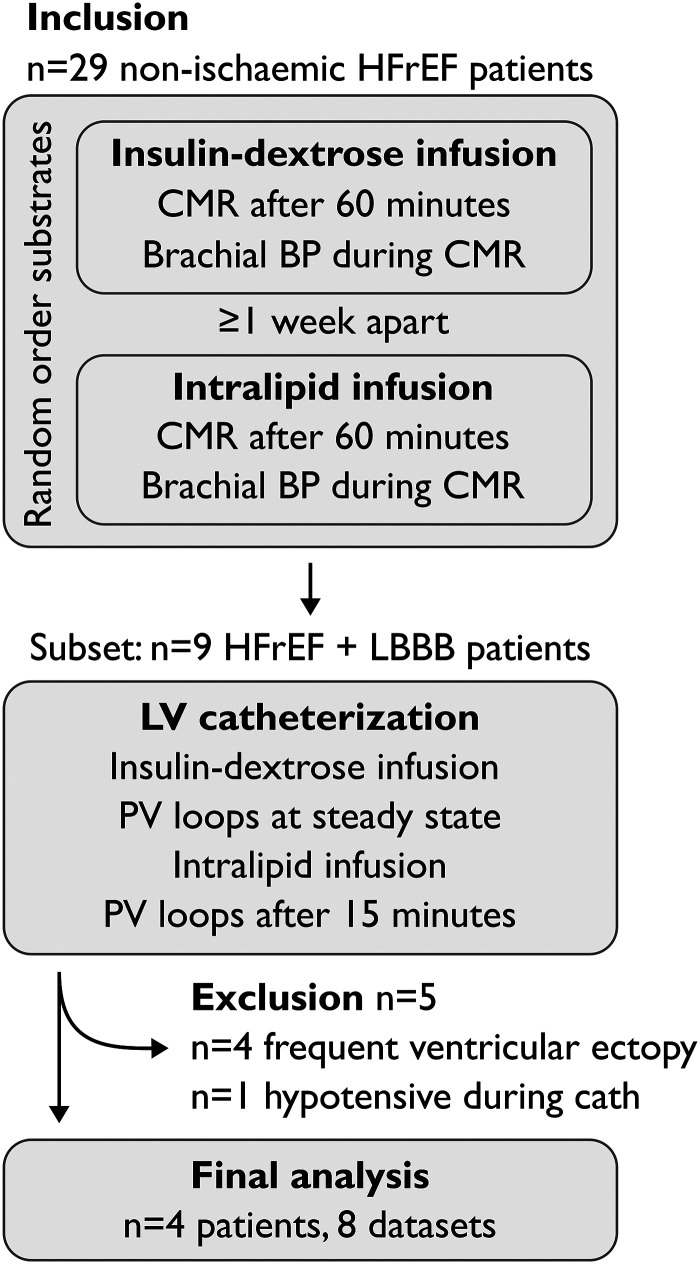
Methods and results: Four heart failure patients with EF < 35% and LV dyssynchrony underwent cardiovascular magnetic resonance (CMR) imaging and subsequent LV catheterization with sequential administration of two different intravenous metabolic substrate infusions (insulin/dextrose and lipid emulsion), producing eight datasets at different haemodynamic states. Pressure-volume loops were computed from CMR volumes combined with (i) a time-varying elastance function scaled to brachial blood pressure and temporally stretched to match volume data, or (ii) invasive pressures averaged from 19 to 30 sampled beats. Method comparison was conducted using linear regression and Bland-Altman analysis. Non-invasively derived PV loop parameters demonstrated high correlation and low bias when compared to invasive data for stroke work (R2 = 0.96, P < 0.0001, bias 4.6%), potential energy (R2 = 0.83, P = 0.001, bias 1.5%), end-systolic pressure-volume relationship (R2 = 0.89, P = 0.0004, bias 5.8%), ventricular efficiency (R2 = 0.98, P < 0.0001, bias 0.8%), arterial elastance (R2 = 0.88, P = 0.0006, bias -8.0%), mean external power (R2 = 0.92, P = 0.0002, bias 4.4%), and energy per ejected volume (R2 = 0.89, P = 0.0001, bias 3.7%). Variations in estimated end-diastolic pressure did not significantly affect results (P > 0.05 for all). Intraobserver analysis after one year demonstrated 0.9-3.4% bias for LV volumetry and 0.2-5.4% for PV loop-derived parameters.
Conclusion: Pressure-volume loops can be precisely and accurately computed from CMR imaging and brachial cuff blood pressure in humans.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
