Florentina M.E. Pinckaers , Magretha M.Q. Robbe , Susanne G.H. Olthuis , Hieronymus D. Boogaarts , Wim H. van Zwam , Robert J. van Oostenbrugge , Alida A. Postma
{"title":"急性缺血性脑卒中血管内治疗后立即颅内出血的双能CT预后意义。","authors":"Florentina M.E. Pinckaers , Magretha M.Q. Robbe , Susanne G.H. Olthuis , Hieronymus D. Boogaarts , Wim H. van Zwam , Robert J. van Oostenbrugge , Alida A. Postma","doi":"10.1016/j.neurad.2023.11.003","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><p>To describe the incidence, risk factors, and prognostic relevance of intracranial haemorrhage (ICH) immediately after endovascular treatment (EVT) for ischaemic stroke in the anterior circulation.</p></div><div><h3>Methods</h3><p>EVT records from 2010 to 2019 were screened. Included patients underwent DECT within 3h post-EVT. Virtual native reconstructions were evaluated for ICH according to the Heidelberg criteria and grouped into Heidelberg classes (HCs): [HC1] haemorrhagic infarction (HI)1, HI2 and parenchymal haematoma (PH)1; [HC2] PH2; [HC3] i.a. intraventricular and subarachnoid haemorrhage. If ICH corresponding to multiple HCs was observed, we assumed that the (largest) parenchymal ICH would have the greatest prognostic impact. Hence, a single HC was attributed by the following order of severity: HC2, HC1, HC3. The primary outcome was the modified Rankin Scale (mRS) at 90 days. The effect of asymptomatic ICH (aICH) and symptomatic ICH (sICH) of (1) HC1 or HC2 and (2) HC3 on patient outcomes was evaluated with multivariable regression after multiple imputation.</p></div><div><h3>Results</h3><p>Out of 651 records, 498 patients were included. Eighty-one (16%) patients showed ICH on post-EVT DECT, of which 19 were classified as HC1 (21% symptomatic), 6 as HC2 (100% symptomatic), and 56 as HC3 (14% symptomatic). ICH development was mainly associated with unfavourable procedural characteristics. Both aICH and sICH of HC1 or HC2 were associated with the mRS (aICH: adjusted [a]cOR 4.92, 95%CI [1.48–16.35]; sICH: acOR 12.97, 95%CI [2.39–70.26]) and mortality (aICH: aOR 10.08, 95%CI [2.48–40.88]; sICH: aOR 9.92, 95%CI [1.48–66.31]). Likewise, sICH of HC3 was associated with the mRS and mortality (acOR 19.91, 95%CI [4.03–98.35], and aOR 13.23, 95%CI [2.27–77.18], respectively). aICH of HC3 was not significantly associated with the mRS or mortality (acOR 0.87, 95%CI [0.48–1.57], and cOR 0.84, 95%CI [0.32–2.20], respectively).</p></div><div><h3>Conclusions</h3><p>Immediate post-EVT ICH is a frequent finding. Except for aICH of HC3, any ICH is associated with poor long-term clinical outcomes.</p></div>","PeriodicalId":50115,"journal":{"name":"Journal of Neuroradiology","volume":"51 4","pages":"Article 101168"},"PeriodicalIF":3.3000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S0150986123002651/pdfft?md5=82b99bc7242f5935dd2946936d104c9a&pid=1-s2.0-S0150986123002651-main.pdf","citationCount":"0","resultStr":"{\"title\":\"Prognostic implications of intracranial haemorrhage on dual-energy CT immediately following endovascular treatment for acute ischemic stroke\",\"authors\":\"Florentina M.E. Pinckaers , Magretha M.Q. Robbe , Susanne G.H. Olthuis , Hieronymus D. Boogaarts , Wim H. van Zwam , Robert J. van Oostenbrugge , Alida A. Postma\",\"doi\":\"10.1016/j.neurad.2023.11.003\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Objective</h3><p>To describe the incidence, risk factors, and prognostic relevance of intracranial haemorrhage (ICH) immediately after endovascular treatment (EVT) for ischaemic stroke in the anterior circulation.</p></div><div><h3>Methods</h3><p>EVT records from 2010 to 2019 were screened. Included patients underwent DECT within 3h post-EVT. Virtual native reconstructions were evaluated for ICH according to the Heidelberg criteria and grouped into Heidelberg classes (HCs): [HC1] haemorrhagic infarction (HI)1, HI2 and parenchymal haematoma (PH)1; [HC2] PH2; [HC3] i.a. intraventricular and subarachnoid haemorrhage. If ICH corresponding to multiple HCs was observed, we assumed that the (largest) parenchymal ICH would have the greatest prognostic impact. Hence, a single HC was attributed by the following order of severity: HC2, HC1, HC3. The primary outcome was the modified Rankin Scale (mRS) at 90 days. The effect of asymptomatic ICH (aICH) and symptomatic ICH (sICH) of (1) HC1 or HC2 and (2) HC3 on patient outcomes was evaluated with multivariable regression after multiple imputation.</p></div><div><h3>Results</h3><p>Out of 651 records, 498 patients were included. Eighty-one (16%) patients showed ICH on post-EVT DECT, of which 19 were classified as HC1 (21% symptomatic), 6 as HC2 (100% symptomatic), and 56 as HC3 (14% symptomatic). ICH development was mainly associated with unfavourable procedural characteristics. Both aICH and sICH of HC1 or HC2 were associated with the mRS (aICH: adjusted [a]cOR 4.92, 95%CI [1.48–16.35]; sICH: acOR 12.97, 95%CI [2.39–70.26]) and mortality (aICH: aOR 10.08, 95%CI [2.48–40.88]; sICH: aOR 9.92, 95%CI [1.48–66.31]). Likewise, sICH of HC3 was associated with the mRS and mortality (acOR 19.91, 95%CI [4.03–98.35], and aOR 13.23, 95%CI [2.27–77.18], respectively). aICH of HC3 was not significantly associated with the mRS or mortality (acOR 0.87, 95%CI [0.48–1.57], and cOR 0.84, 95%CI [0.32–2.20], respectively).</p></div><div><h3>Conclusions</h3><p>Immediate post-EVT ICH is a frequent finding. Except for aICH of HC3, any ICH is associated with poor long-term clinical outcomes.</p></div>\",\"PeriodicalId\":50115,\"journal\":{\"name\":\"Journal of Neuroradiology\",\"volume\":\"51 4\",\"pages\":\"Article 101168\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2024-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.sciencedirect.com/science/article/pii/S0150986123002651/pdfft?md5=82b99bc7242f5935dd2946936d104c9a&pid=1-s2.0-S0150986123002651-main.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Neuroradiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S0150986123002651\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/11/19 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Neuroradiology","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0150986123002651","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/11/19 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Prognostic implications of intracranial haemorrhage on dual-energy CT immediately following endovascular treatment for acute ischemic stroke
Objective
To describe the incidence, risk factors, and prognostic relevance of intracranial haemorrhage (ICH) immediately after endovascular treatment (EVT) for ischaemic stroke in the anterior circulation.
Methods
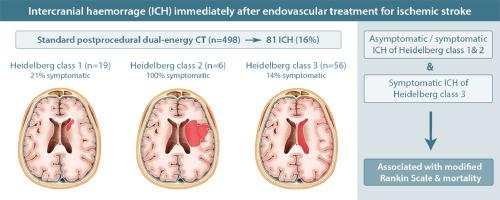
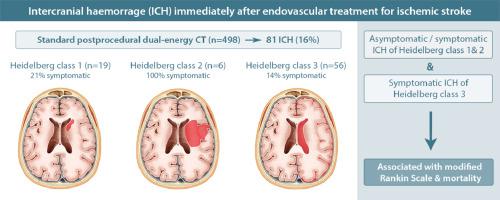
EVT records from 2010 to 2019 were screened. Included patients underwent DECT within 3h post-EVT. Virtual native reconstructions were evaluated for ICH according to the Heidelberg criteria and grouped into Heidelberg classes (HCs): [HC1] haemorrhagic infarction (HI)1, HI2 and parenchymal haematoma (PH)1; [HC2] PH2; [HC3] i.a. intraventricular and subarachnoid haemorrhage. If ICH corresponding to multiple HCs was observed, we assumed that the (largest) parenchymal ICH would have the greatest prognostic impact. Hence, a single HC was attributed by the following order of severity: HC2, HC1, HC3. The primary outcome was the modified Rankin Scale (mRS) at 90 days. The effect of asymptomatic ICH (aICH) and symptomatic ICH (sICH) of (1) HC1 or HC2 and (2) HC3 on patient outcomes was evaluated with multivariable regression after multiple imputation.
Results
Out of 651 records, 498 patients were included. Eighty-one (16%) patients showed ICH on post-EVT DECT, of which 19 were classified as HC1 (21% symptomatic), 6 as HC2 (100% symptomatic), and 56 as HC3 (14% symptomatic). ICH development was mainly associated with unfavourable procedural characteristics. Both aICH and sICH of HC1 or HC2 were associated with the mRS (aICH: adjusted [a]cOR 4.92, 95%CI [1.48–16.35]; sICH: acOR 12.97, 95%CI [2.39–70.26]) and mortality (aICH: aOR 10.08, 95%CI [2.48–40.88]; sICH: aOR 9.92, 95%CI [1.48–66.31]). Likewise, sICH of HC3 was associated with the mRS and mortality (acOR 19.91, 95%CI [4.03–98.35], and aOR 13.23, 95%CI [2.27–77.18], respectively). aICH of HC3 was not significantly associated with the mRS or mortality (acOR 0.87, 95%CI [0.48–1.57], and cOR 0.84, 95%CI [0.32–2.20], respectively).
Conclusions
Immediate post-EVT ICH is a frequent finding. Except for aICH of HC3, any ICH is associated with poor long-term clinical outcomes.
期刊介绍:
The Journal of Neuroradiology is a peer-reviewed journal, publishing worldwide clinical and basic research in the field of diagnostic and Interventional neuroradiology, translational and molecular neuroimaging, and artificial intelligence in neuroradiology.
The Journal of Neuroradiology considers for publication articles, reviews, technical notes and letters to the editors (correspondence section), provided that the methodology and scientific content are of high quality, and that the results will have substantial clinical impact and/or physiological importance.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
