{"title":"周炎与植体治疗1例。","authors":"Jonathan H. Do, Charles M. Cobb","doi":"10.1002/cap.10271","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>A previous case study reported periimplantitis and concomitant perigraftitis of a second implant placed at a site that had alveolar ridge preservation three decades earlier. Infection at the site persisted 4 months after implant removal by flapless implant reversal. A flap was subsequently reflected, the grafted bone was removed, and a second alveolar ridge preservation was performed with a freeze-dried bone allograft. The publication reported infection resolved, and the site healed uneventfully. However, it is unknown if placement of another implant at the site would be successful. The purpose of this paper is to report on the findings at surgical reentry and outcome of the third implant.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Eleven months after the second alveolar ridge preservation, the site was reentered. The bone graft was found to be partially soft tissue encapsulated. All encapsulated graft materials and soft tissue were removed. An implant was placed, and the alveolar defect was grafted with a demineralized bone allograft. Seventeen months after implant placement, a buccal free gingival graft was performed during which the crestal bone adjacent to the implant was found to be hard and corticated. The implant was deemed to be osseointegrated and restored after soft tissue healing.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Twenty-five months after implant placement, the third implant remained functional and asymptomatic with the peri-implant bone exhibiting normal trabeculation.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Implant therapy can be successful following treatment and resolution of perigraftitis.</p>\n </section>\n \n <section>\n \n <h3> Key points</h3>\n \n <div>\n <ul>\n \n <li>\n <p>Perigraftitis may play a contributing role in the biologic complications of implants that have been placed into grafted bone.</p>\n </li>\n \n <li>\n <p>Perigraftitis may be successfully resolved by completely removing all grafted bone.</p>\n </li>\n \n <li>\n <p>Once perigraftitis has been eliminated, an implant may be successfully placed.</p>\n </li>\n </ul>\n </div>\n </section>\n </div>","PeriodicalId":55950,"journal":{"name":"Clinical Advances in Periodontics","volume":"14 3","pages":"172-179"},"PeriodicalIF":0.9000,"publicationDate":"2023-11-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cap.10271","citationCount":"0","resultStr":"{\"title\":\"Perigraftitis and implant therapy: A case report\",\"authors\":\"Jonathan H. Do, Charles M. Cobb\",\"doi\":\"10.1002/cap.10271\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>A previous case study reported periimplantitis and concomitant perigraftitis of a second implant placed at a site that had alveolar ridge preservation three decades earlier. Infection at the site persisted 4 months after implant removal by flapless implant reversal. A flap was subsequently reflected, the grafted bone was removed, and a second alveolar ridge preservation was performed with a freeze-dried bone allograft. The publication reported infection resolved, and the site healed uneventfully. However, it is unknown if placement of another implant at the site would be successful. The purpose of this paper is to report on the findings at surgical reentry and outcome of the third implant.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>Eleven months after the second alveolar ridge preservation, the site was reentered. The bone graft was found to be partially soft tissue encapsulated. All encapsulated graft materials and soft tissue were removed. An implant was placed, and the alveolar defect was grafted with a demineralized bone allograft. Seventeen months after implant placement, a buccal free gingival graft was performed during which the crestal bone adjacent to the implant was found to be hard and corticated. The implant was deemed to be osseointegrated and restored after soft tissue healing.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Twenty-five months after implant placement, the third implant remained functional and asymptomatic with the peri-implant bone exhibiting normal trabeculation.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Implant therapy can be successful following treatment and resolution of perigraftitis.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Key points</h3>\\n \\n <div>\\n <ul>\\n \\n <li>\\n <p>Perigraftitis may play a contributing role in the biologic complications of implants that have been placed into grafted bone.</p>\\n </li>\\n \\n <li>\\n <p>Perigraftitis may be successfully resolved by completely removing all grafted bone.</p>\\n </li>\\n \\n <li>\\n <p>Once perigraftitis has been eliminated, an implant may be successfully placed.</p>\\n </li>\\n </ul>\\n </div>\\n </section>\\n </div>\",\"PeriodicalId\":55950,\"journal\":{\"name\":\"Clinical Advances in Periodontics\",\"volume\":\"14 3\",\"pages\":\"172-179\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2023-11-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cap.10271\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Advances in Periodontics\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://aap.onlinelibrary.wiley.com/doi/10.1002/cap.10271\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"DENTISTRY, ORAL SURGERY & MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Advances in Periodontics","FirstCategoryId":"1085","ListUrlMain":"https://aap.onlinelibrary.wiley.com/doi/10.1002/cap.10271","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"DENTISTRY, ORAL SURGERY & MEDICINE","Score":null,"Total":0}
A previous case study reported periimplantitis and concomitant perigraftitis of a second implant placed at a site that had alveolar ridge preservation three decades earlier. Infection at the site persisted 4 months after implant removal by flapless implant reversal. A flap was subsequently reflected, the grafted bone was removed, and a second alveolar ridge preservation was performed with a freeze-dried bone allograft. The publication reported infection resolved, and the site healed uneventfully. However, it is unknown if placement of another implant at the site would be successful. The purpose of this paper is to report on the findings at surgical reentry and outcome of the third implant.
Methods
Eleven months after the second alveolar ridge preservation, the site was reentered. The bone graft was found to be partially soft tissue encapsulated. All encapsulated graft materials and soft tissue were removed. An implant was placed, and the alveolar defect was grafted with a demineralized bone allograft. Seventeen months after implant placement, a buccal free gingival graft was performed during which the crestal bone adjacent to the implant was found to be hard and corticated. The implant was deemed to be osseointegrated and restored after soft tissue healing.
Results
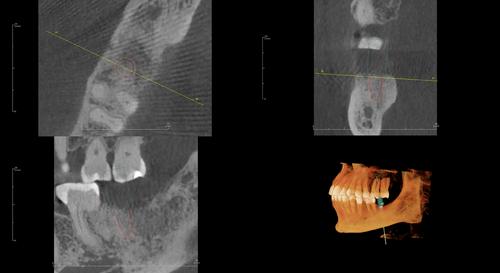
Twenty-five months after implant placement, the third implant remained functional and asymptomatic with the peri-implant bone exhibiting normal trabeculation.
Conclusions
Implant therapy can be successful following treatment and resolution of perigraftitis.
Key points
Perigraftitis may play a contributing role in the biologic complications of implants that have been placed into grafted bone.
Perigraftitis may be successfully resolved by completely removing all grafted bone.
Once perigraftitis has been eliminated, an implant may be successfully placed.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
