Sally A. Santen MD, PhD, Robin R. Hemphill MD, MPH, Martin Pusic MD, PhD, Stephen John Cico MD, MEd, Meg Wolff MD, MHPE, Chris Merritt MD, MHPE
{"title":"我们对病人的责任是:要么保持能力,要么停止行医。","authors":"Sally A. Santen MD, PhD, Robin R. Hemphill MD, MPH, Martin Pusic MD, PhD, Stephen John Cico MD, MEd, Meg Wolff MD, MHPE, Chris Merritt MD, MHPE","doi":"10.1002/aet2.10916","DOIUrl":null,"url":null,"abstract":"<p>On March 30, 1981, after President Reagan was shot in the chest by John Hinckley, he was taken to the hospital and required a chest tube. Rumor has it, a department chair stepped up to perform the procedure, hitting the intercostal artery in the process, necessitating a blood transfusion. As well-trained interns know, you place a chest tube above the rib; when you go below the rib, you may hit the intercostal artery. Although, this story may be urban legend, it resonates because it speaks to an important lesson—if you need a procedure, you want the person who does it the most frequently—the senior resident, junior attending, or specialized consultant. Most likely you do not want the department chair, associate dean, physician-scientist, part-time physician moving to retirement, or others with less clinical practice. Medical errors are common. Procedural complications are an important cause of adverse events, resulting in patient discomfort, longer hospital stays, and higher costs.<span><sup>1</sup></span> These complications result in nearly 10% of hospital-wide adverse events; nearly half are considered preventable.<span><sup>2</sup></span></p><p>For the past several years, our emergency medicine (EM) clinical practice has been about 20% of our time, less than 1 day a week. While we may be reluctant to admit it, the last lumbar puncture any of us performed was over a year ago, our last intubation was perhaps years ago, and a cricothyrotomy was in residency over 25 years ago. We practice in teaching hospitals, and have supervised these procedures, but have not recently performed them. While we believe that we are in equipoise, providing excellent patient care based on years of experience and balancing infrequent procedural performance, could we still do these procedures? Probably yes, maybe not perfectly, and at what risk to the patient? Yet, we still practice, and we accept the responsibility to provide optimal care for our patients. Moreover, our identity as competent emergency physicians is important and contributes to our professional credibility.</p><p>Emergency physicians have a continuous responsibility to maintain competency. Yet medical care is rapidly changing; new procedures such as ultrasound-guided nerve blocks become standard of care. There are new diseases such as COVID and new treatments such as thrombectomy for stroke. Further, about half of patients' medications did not exist in medical school and may not know the interactions and side effects. In addition, there are numerous high-acuity low opportunity (HALO) procedures (e.g., thoracotomy, lateral canthotomy, and transvenous pacer)<span><sup>3</sup></span> and HALO patient presentations (e.g., neonatal shock, thyroid storm). So how do EM physicians maintain their knowledge and competencies, much less extend these into emerging procedures, medications, diseases, and treatments?</p><p>Maintenance of skills is important; crucial questions remain unanswered. <i>What must EM physicians be competent in</i>,<span><sup>4</sup></span> <i>for how long, and how?</i> Where an expansive range of competencies are considered centrally important, it is clear not every practitioner maintains every competency. Achieving, assuring, and maintaining competency comes at a cost in time, effort, and perseverance for the individual and the system.</p><p>Medical training cycles through periods of rapid learning with large gains in performance and expertise, especially during transitions to clerkship, residency, and practice (Figure 1).<span><sup>5, 6</sup></span> Learning is accelerated by spaced repetition,<span><sup>7</sup></span> interleaving,<span><sup>8</sup></span> deliberate practice with feedback,<span><sup>9</sup></span> and metacognitive techniques such as informed self-assessment<span><sup>10</sup></span> and deep reflection.<span><sup>11</sup></span> When formal training ceases, expert performance can eventually degrade. The rate of forgetting depends on a number of factors including the skill complexity, opportunities for practice, and system support.<span><sup>5, 6</sup></span> Strong learning techniques can delay or lessen the forgetting curve, as does continued exposure through practice.</p><p>Training for adaptive expertise mitigates some of forgetting effects. Educational designs emphasizing deep mechanistic understanding and an ability to cope with meaningful variation in patient care allows a physician to more ably approach problems for which they do not have a fully routinized approach.<span><sup>12</sup></span> This acknowledges that a procedure that one provider has fully routinized, another provider might need to invoke their ability to innovate in the moment (i.e., adapt).<span><sup>6</sup></span> However, while experience may provide better adaptive approaches, this can only take them so far, as our President Reagan chest tube story shows.</p><p>In this perspective we raise questions of forgetting curves and the responsibility of managing procedural skills and clinical competency. Can the balance tip in a way that results in harm for patients? And what can we do to mitigate and protect? We propose four approaches.</p><p>First, there is the external mandate for lifelong learning, continuing medical education credits for renewal of licensure, and the sticky problem of maintenance of certification and recertification examinations.<span><sup>13</sup></span> While these are often unpopular and potentially ineffective, the underlying principle is solid. Physicians will forget what is not used, need to refresh core knowledge, and must learn the new knowledge and skills. Essential in this process is that physicians become master adaptive learners<span><sup>14, 15</sup></span> who must recognize what they do not know, identify gaps, plan, and implement effective learning. Beyond mandatory CME and recertification, EM physicians have a responsibility to continue to learn for the benefit of their patients.</p><p>The second approach invokes the responsibility of <i>all</i> physicians to maintain competency by retraining specifically for HALO and new procedures. Simulation is widely available but may not be used by practicing physicians and may not be considered part of a simulation centers' budget and mission. These opportunities allow physicians to refresh their procedural memory as well as develop familiarity with new equipment and methods. Some departments have faculty- specific voluntary procedural training or mandate training, such as annual procedural sedation certification.<span><sup>16, 17</sup></span> There are national EM courses in domains such as airway, ultrasound, and trauma that facilitate learning.</p><p>The third approach is that physicians can choose to limit their practice by working in settings where there is less exposure to the procedures or content in which they are no longer expert. EM physicians can work in lower acuity areas or locations with double coverage with reliance on colleagues as needed, locations with support of a procedural or ED/intensive care unit team, or adult hospitals (allow pediatric skills to decay). These options leverage alignment with systems-based approaches that maximize collective competence.<span><sup>18</sup></span> The optimal solution is likely to differ between settings and EM providers.<span><sup>19</sup></span></p><p>Finally, and perhaps most importantly, is the twin-mirror of self-assessment and reflection. Self-assessment can be poor, as shown by Dunning and Kruger's paper “Unskilled and unaware: How difficulties in recognizing one's own incompetence lead to inflated self-assessments.”<span><sup>20</sup></span> Physicians may not realize or admit that they have lost competency. This threat to our professional identity—that of the competent physician—creates internal conflict. Emergency physicians must seek external metrics to provide informed self-assessment.<span><sup>10, 21</sup></span> This requires us to understand how we ascend to expertise—the time, practice, and self-challenge that achieves peak performance. We must then also understand that when we cease to do the things that maintain that expertise, our experience can take us only so far, and performance may decline unless deliberate retraining steps are taken.</p><p>In the face of forgetting curves, HALO procedures and cases, and expanding knowledge there is a responsibility of the medical profession to ensure that patients come first.<span><sup>22</sup></span> We must place patient safety first and take this responsibility to self-assess and self-reflect—and importantly, to <i>change</i>—either ourselves or our practice if we recognize that the safety of patients is threatened by our decay in competence.</p><p>More importantly, data-informed systems must be created to ensure that the patient safety/physician competency tension is not driven solely by the individual. Most of us know a colleague whose care we do not trust for patients or our family members or who we dread signing out to.<span><sup>23-25</sup></span> The system must be intentional about identifying these providers and working to improve their care (Table 1). The chair in the opening story should not have been in the situation to place a chest tube if he had not performed them regularly. Health care systems need to develop proactive processes of continuous review of physician competency such as errors, near-miss, peer concerns, low volume of specific cases, safety events, complications, patient-reported outcomes, and patient and staff complaints. These metrics might launch a more extensive review of practice including peer assessments, direct observation, chart review, knowledge analysis, cognitive testing, procedural testing, and other methods of competency assessment.<span><sup>26</sup></span> The challenge is that this may feel punitive<span><sup>27</sup></span> and colleagues and systems are hesitant to trigger such a review out of collegial compassion and concern that there is not sufficient “evidence.” We need a proactive system that faces these issues directly with regular reviews of practice or mandatory competency assessments. Beyond surveillance, the health system must provide proactive, individualized, transparent training opportunities that mitigate skill attrition before it takes hold. Further, there must be recognition of the time and resources it takes to retain skills and this should be supported by health systems. Our responsibility is to maintain competency. The locus of responsibility for ensuring competency must be shared between the individual and the health system to provide safe and effective care for patients.</p><p>The authors declare no conflicts of interest. Robin Hemphill is an employee of the Veteran's Health Administration (VHA). These views are her own and do not represent the views of the VHA.</p>","PeriodicalId":37032,"journal":{"name":"AEM Education and Training","volume":"7 6","pages":""},"PeriodicalIF":1.6000,"publicationDate":"2023-11-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10664403/pdf/","citationCount":"1","resultStr":"{\"title\":\"Our responsibility to patients: Maintain competency or … stop practicing\",\"authors\":\"Sally A. Santen MD, PhD, Robin R. Hemphill MD, MPH, Martin Pusic MD, PhD, Stephen John Cico MD, MEd, Meg Wolff MD, MHPE, Chris Merritt MD, MHPE\",\"doi\":\"10.1002/aet2.10916\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>On March 30, 1981, after President Reagan was shot in the chest by John Hinckley, he was taken to the hospital and required a chest tube. Rumor has it, a department chair stepped up to perform the procedure, hitting the intercostal artery in the process, necessitating a blood transfusion. As well-trained interns know, you place a chest tube above the rib; when you go below the rib, you may hit the intercostal artery. Although, this story may be urban legend, it resonates because it speaks to an important lesson—if you need a procedure, you want the person who does it the most frequently—the senior resident, junior attending, or specialized consultant. Most likely you do not want the department chair, associate dean, physician-scientist, part-time physician moving to retirement, or others with less clinical practice. Medical errors are common. Procedural complications are an important cause of adverse events, resulting in patient discomfort, longer hospital stays, and higher costs.<span><sup>1</sup></span> These complications result in nearly 10% of hospital-wide adverse events; nearly half are considered preventable.<span><sup>2</sup></span></p><p>For the past several years, our emergency medicine (EM) clinical practice has been about 20% of our time, less than 1 day a week. While we may be reluctant to admit it, the last lumbar puncture any of us performed was over a year ago, our last intubation was perhaps years ago, and a cricothyrotomy was in residency over 25 years ago. We practice in teaching hospitals, and have supervised these procedures, but have not recently performed them. While we believe that we are in equipoise, providing excellent patient care based on years of experience and balancing infrequent procedural performance, could we still do these procedures? Probably yes, maybe not perfectly, and at what risk to the patient? Yet, we still practice, and we accept the responsibility to provide optimal care for our patients. Moreover, our identity as competent emergency physicians is important and contributes to our professional credibility.</p><p>Emergency physicians have a continuous responsibility to maintain competency. Yet medical care is rapidly changing; new procedures such as ultrasound-guided nerve blocks become standard of care. There are new diseases such as COVID and new treatments such as thrombectomy for stroke. Further, about half of patients' medications did not exist in medical school and may not know the interactions and side effects. In addition, there are numerous high-acuity low opportunity (HALO) procedures (e.g., thoracotomy, lateral canthotomy, and transvenous pacer)<span><sup>3</sup></span> and HALO patient presentations (e.g., neonatal shock, thyroid storm). So how do EM physicians maintain their knowledge and competencies, much less extend these into emerging procedures, medications, diseases, and treatments?</p><p>Maintenance of skills is important; crucial questions remain unanswered. <i>What must EM physicians be competent in</i>,<span><sup>4</sup></span> <i>for how long, and how?</i> Where an expansive range of competencies are considered centrally important, it is clear not every practitioner maintains every competency. Achieving, assuring, and maintaining competency comes at a cost in time, effort, and perseverance for the individual and the system.</p><p>Medical training cycles through periods of rapid learning with large gains in performance and expertise, especially during transitions to clerkship, residency, and practice (Figure 1).<span><sup>5, 6</sup></span> Learning is accelerated by spaced repetition,<span><sup>7</sup></span> interleaving,<span><sup>8</sup></span> deliberate practice with feedback,<span><sup>9</sup></span> and metacognitive techniques such as informed self-assessment<span><sup>10</sup></span> and deep reflection.<span><sup>11</sup></span> When formal training ceases, expert performance can eventually degrade. The rate of forgetting depends on a number of factors including the skill complexity, opportunities for practice, and system support.<span><sup>5, 6</sup></span> Strong learning techniques can delay or lessen the forgetting curve, as does continued exposure through practice.</p><p>Training for adaptive expertise mitigates some of forgetting effects. Educational designs emphasizing deep mechanistic understanding and an ability to cope with meaningful variation in patient care allows a physician to more ably approach problems for which they do not have a fully routinized approach.<span><sup>12</sup></span> This acknowledges that a procedure that one provider has fully routinized, another provider might need to invoke their ability to innovate in the moment (i.e., adapt).<span><sup>6</sup></span> However, while experience may provide better adaptive approaches, this can only take them so far, as our President Reagan chest tube story shows.</p><p>In this perspective we raise questions of forgetting curves and the responsibility of managing procedural skills and clinical competency. Can the balance tip in a way that results in harm for patients? And what can we do to mitigate and protect? We propose four approaches.</p><p>First, there is the external mandate for lifelong learning, continuing medical education credits for renewal of licensure, and the sticky problem of maintenance of certification and recertification examinations.<span><sup>13</sup></span> While these are often unpopular and potentially ineffective, the underlying principle is solid. Physicians will forget what is not used, need to refresh core knowledge, and must learn the new knowledge and skills. Essential in this process is that physicians become master adaptive learners<span><sup>14, 15</sup></span> who must recognize what they do not know, identify gaps, plan, and implement effective learning. Beyond mandatory CME and recertification, EM physicians have a responsibility to continue to learn for the benefit of their patients.</p><p>The second approach invokes the responsibility of <i>all</i> physicians to maintain competency by retraining specifically for HALO and new procedures. Simulation is widely available but may not be used by practicing physicians and may not be considered part of a simulation centers' budget and mission. These opportunities allow physicians to refresh their procedural memory as well as develop familiarity with new equipment and methods. Some departments have faculty- specific voluntary procedural training or mandate training, such as annual procedural sedation certification.<span><sup>16, 17</sup></span> There are national EM courses in domains such as airway, ultrasound, and trauma that facilitate learning.</p><p>The third approach is that physicians can choose to limit their practice by working in settings where there is less exposure to the procedures or content in which they are no longer expert. EM physicians can work in lower acuity areas or locations with double coverage with reliance on colleagues as needed, locations with support of a procedural or ED/intensive care unit team, or adult hospitals (allow pediatric skills to decay). These options leverage alignment with systems-based approaches that maximize collective competence.<span><sup>18</sup></span> The optimal solution is likely to differ between settings and EM providers.<span><sup>19</sup></span></p><p>Finally, and perhaps most importantly, is the twin-mirror of self-assessment and reflection. Self-assessment can be poor, as shown by Dunning and Kruger's paper “Unskilled and unaware: How difficulties in recognizing one's own incompetence lead to inflated self-assessments.”<span><sup>20</sup></span> Physicians may not realize or admit that they have lost competency. This threat to our professional identity—that of the competent physician—creates internal conflict. Emergency physicians must seek external metrics to provide informed self-assessment.<span><sup>10, 21</sup></span> This requires us to understand how we ascend to expertise—the time, practice, and self-challenge that achieves peak performance. We must then also understand that when we cease to do the things that maintain that expertise, our experience can take us only so far, and performance may decline unless deliberate retraining steps are taken.</p><p>In the face of forgetting curves, HALO procedures and cases, and expanding knowledge there is a responsibility of the medical profession to ensure that patients come first.<span><sup>22</sup></span> We must place patient safety first and take this responsibility to self-assess and self-reflect—and importantly, to <i>change</i>—either ourselves or our practice if we recognize that the safety of patients is threatened by our decay in competence.</p><p>More importantly, data-informed systems must be created to ensure that the patient safety/physician competency tension is not driven solely by the individual. Most of us know a colleague whose care we do not trust for patients or our family members or who we dread signing out to.<span><sup>23-25</sup></span> The system must be intentional about identifying these providers and working to improve their care (Table 1). The chair in the opening story should not have been in the situation to place a chest tube if he had not performed them regularly. Health care systems need to develop proactive processes of continuous review of physician competency such as errors, near-miss, peer concerns, low volume of specific cases, safety events, complications, patient-reported outcomes, and patient and staff complaints. These metrics might launch a more extensive review of practice including peer assessments, direct observation, chart review, knowledge analysis, cognitive testing, procedural testing, and other methods of competency assessment.<span><sup>26</sup></span> The challenge is that this may feel punitive<span><sup>27</sup></span> and colleagues and systems are hesitant to trigger such a review out of collegial compassion and concern that there is not sufficient “evidence.” We need a proactive system that faces these issues directly with regular reviews of practice or mandatory competency assessments. Beyond surveillance, the health system must provide proactive, individualized, transparent training opportunities that mitigate skill attrition before it takes hold. Further, there must be recognition of the time and resources it takes to retain skills and this should be supported by health systems. Our responsibility is to maintain competency. The locus of responsibility for ensuring competency must be shared between the individual and the health system to provide safe and effective care for patients.</p><p>The authors declare no conflicts of interest. Robin Hemphill is an employee of the Veteran's Health Administration (VHA). These views are her own and do not represent the views of the VHA.</p>\",\"PeriodicalId\":37032,\"journal\":{\"name\":\"AEM Education and Training\",\"volume\":\"7 6\",\"pages\":\"\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2023-11-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10664403/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"AEM Education and Training\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/aet2.10916\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"EDUCATION, SCIENTIFIC DISCIPLINES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"AEM Education and Training","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/aet2.10916","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EDUCATION, SCIENTIFIC DISCIPLINES","Score":null,"Total":0}
Our responsibility to patients: Maintain competency or … stop practicing
On March 30, 1981, after President Reagan was shot in the chest by John Hinckley, he was taken to the hospital and required a chest tube. Rumor has it, a department chair stepped up to perform the procedure, hitting the intercostal artery in the process, necessitating a blood transfusion. As well-trained interns know, you place a chest tube above the rib; when you go below the rib, you may hit the intercostal artery. Although, this story may be urban legend, it resonates because it speaks to an important lesson—if you need a procedure, you want the person who does it the most frequently—the senior resident, junior attending, or specialized consultant. Most likely you do not want the department chair, associate dean, physician-scientist, part-time physician moving to retirement, or others with less clinical practice. Medical errors are common. Procedural complications are an important cause of adverse events, resulting in patient discomfort, longer hospital stays, and higher costs.1 These complications result in nearly 10% of hospital-wide adverse events; nearly half are considered preventable.2
For the past several years, our emergency medicine (EM) clinical practice has been about 20% of our time, less than 1 day a week. While we may be reluctant to admit it, the last lumbar puncture any of us performed was over a year ago, our last intubation was perhaps years ago, and a cricothyrotomy was in residency over 25 years ago. We practice in teaching hospitals, and have supervised these procedures, but have not recently performed them. While we believe that we are in equipoise, providing excellent patient care based on years of experience and balancing infrequent procedural performance, could we still do these procedures? Probably yes, maybe not perfectly, and at what risk to the patient? Yet, we still practice, and we accept the responsibility to provide optimal care for our patients. Moreover, our identity as competent emergency physicians is important and contributes to our professional credibility.
Emergency physicians have a continuous responsibility to maintain competency. Yet medical care is rapidly changing; new procedures such as ultrasound-guided nerve blocks become standard of care. There are new diseases such as COVID and new treatments such as thrombectomy for stroke. Further, about half of patients' medications did not exist in medical school and may not know the interactions and side effects. In addition, there are numerous high-acuity low opportunity (HALO) procedures (e.g., thoracotomy, lateral canthotomy, and transvenous pacer)3 and HALO patient presentations (e.g., neonatal shock, thyroid storm). So how do EM physicians maintain their knowledge and competencies, much less extend these into emerging procedures, medications, diseases, and treatments?
Maintenance of skills is important; crucial questions remain unanswered. What must EM physicians be competent in,4for how long, and how? Where an expansive range of competencies are considered centrally important, it is clear not every practitioner maintains every competency. Achieving, assuring, and maintaining competency comes at a cost in time, effort, and perseverance for the individual and the system.
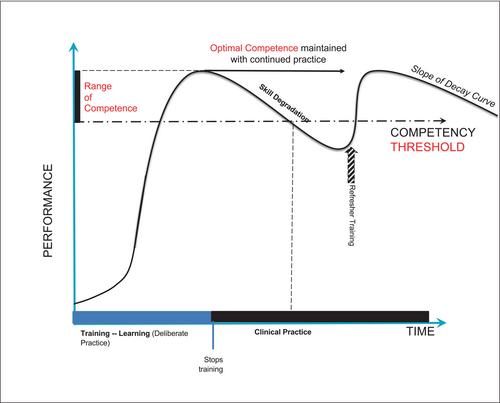
Medical training cycles through periods of rapid learning with large gains in performance and expertise, especially during transitions to clerkship, residency, and practice (Figure 1).5, 6 Learning is accelerated by spaced repetition,7 interleaving,8 deliberate practice with feedback,9 and metacognitive techniques such as informed self-assessment10 and deep reflection.11 When formal training ceases, expert performance can eventually degrade. The rate of forgetting depends on a number of factors including the skill complexity, opportunities for practice, and system support.5, 6 Strong learning techniques can delay or lessen the forgetting curve, as does continued exposure through practice.
Training for adaptive expertise mitigates some of forgetting effects. Educational designs emphasizing deep mechanistic understanding and an ability to cope with meaningful variation in patient care allows a physician to more ably approach problems for which they do not have a fully routinized approach.12 This acknowledges that a procedure that one provider has fully routinized, another provider might need to invoke their ability to innovate in the moment (i.e., adapt).6 However, while experience may provide better adaptive approaches, this can only take them so far, as our President Reagan chest tube story shows.
In this perspective we raise questions of forgetting curves and the responsibility of managing procedural skills and clinical competency. Can the balance tip in a way that results in harm for patients? And what can we do to mitigate and protect? We propose four approaches.
First, there is the external mandate for lifelong learning, continuing medical education credits for renewal of licensure, and the sticky problem of maintenance of certification and recertification examinations.13 While these are often unpopular and potentially ineffective, the underlying principle is solid. Physicians will forget what is not used, need to refresh core knowledge, and must learn the new knowledge and skills. Essential in this process is that physicians become master adaptive learners14, 15 who must recognize what they do not know, identify gaps, plan, and implement effective learning. Beyond mandatory CME and recertification, EM physicians have a responsibility to continue to learn for the benefit of their patients.
The second approach invokes the responsibility of all physicians to maintain competency by retraining specifically for HALO and new procedures. Simulation is widely available but may not be used by practicing physicians and may not be considered part of a simulation centers' budget and mission. These opportunities allow physicians to refresh their procedural memory as well as develop familiarity with new equipment and methods. Some departments have faculty- specific voluntary procedural training or mandate training, such as annual procedural sedation certification.16, 17 There are national EM courses in domains such as airway, ultrasound, and trauma that facilitate learning.
The third approach is that physicians can choose to limit their practice by working in settings where there is less exposure to the procedures or content in which they are no longer expert. EM physicians can work in lower acuity areas or locations with double coverage with reliance on colleagues as needed, locations with support of a procedural or ED/intensive care unit team, or adult hospitals (allow pediatric skills to decay). These options leverage alignment with systems-based approaches that maximize collective competence.18 The optimal solution is likely to differ between settings and EM providers.19
Finally, and perhaps most importantly, is the twin-mirror of self-assessment and reflection. Self-assessment can be poor, as shown by Dunning and Kruger's paper “Unskilled and unaware: How difficulties in recognizing one's own incompetence lead to inflated self-assessments.”20 Physicians may not realize or admit that they have lost competency. This threat to our professional identity—that of the competent physician—creates internal conflict. Emergency physicians must seek external metrics to provide informed self-assessment.10, 21 This requires us to understand how we ascend to expertise—the time, practice, and self-challenge that achieves peak performance. We must then also understand that when we cease to do the things that maintain that expertise, our experience can take us only so far, and performance may decline unless deliberate retraining steps are taken.
In the face of forgetting curves, HALO procedures and cases, and expanding knowledge there is a responsibility of the medical profession to ensure that patients come first.22 We must place patient safety first and take this responsibility to self-assess and self-reflect—and importantly, to change—either ourselves or our practice if we recognize that the safety of patients is threatened by our decay in competence.
More importantly, data-informed systems must be created to ensure that the patient safety/physician competency tension is not driven solely by the individual. Most of us know a colleague whose care we do not trust for patients or our family members or who we dread signing out to.23-25 The system must be intentional about identifying these providers and working to improve their care (Table 1). The chair in the opening story should not have been in the situation to place a chest tube if he had not performed them regularly. Health care systems need to develop proactive processes of continuous review of physician competency such as errors, near-miss, peer concerns, low volume of specific cases, safety events, complications, patient-reported outcomes, and patient and staff complaints. These metrics might launch a more extensive review of practice including peer assessments, direct observation, chart review, knowledge analysis, cognitive testing, procedural testing, and other methods of competency assessment.26 The challenge is that this may feel punitive27 and colleagues and systems are hesitant to trigger such a review out of collegial compassion and concern that there is not sufficient “evidence.” We need a proactive system that faces these issues directly with regular reviews of practice or mandatory competency assessments. Beyond surveillance, the health system must provide proactive, individualized, transparent training opportunities that mitigate skill attrition before it takes hold. Further, there must be recognition of the time and resources it takes to retain skills and this should be supported by health systems. Our responsibility is to maintain competency. The locus of responsibility for ensuring competency must be shared between the individual and the health system to provide safe and effective care for patients.
The authors declare no conflicts of interest. Robin Hemphill is an employee of the Veteran's Health Administration (VHA). These views are her own and do not represent the views of the VHA.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
