{"title":"地塞米松诱导CYP3A活性可能不强,即使在高剂量:从他克莫司共给药的情况下的见解。","authors":"Yoshiyuki Ohno, Toyohito Oriyama, Akira Honda, Mineo Kurokawa, Tappei Takada","doi":"10.1186/s40780-023-00310-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Dexamethasone (DEX) induces CYP3A activity in a concentration-dependent manner. However, no study has examined changes in the blood concentration of CYP3A substrate drugs when DEX is administered at high doses. Herein, we present a case in which tacrolimus (TAC), a typical CYP3A substrate drug, was co-administered with a chemotherapy regimen that included high-dose DEX.</p><p><strong>Case presentation: </strong>A 71-year-old woman underwent liver transplantation for hepatocellular carcinoma 18 years prior to her inclusion in this case study. She was receiving TAC orally at 2 mg/day and had a stable trough blood concentration of approximately 4 ng/mL and a trough blood concentration/dose (C/D) ratio of approximately 2. The patient was diagnosed with post-transplant lymphoproliferative disease (histological type: Burkitt's lymphoma) after admission. Thereafter, the patient received cyclophosphamide-prednisolone (CP), followed by two courses of R-HyperCVAD (rituximab, cyclophosphamide, doxorubicin, vincristine, and DEX) and R-MA (rituximab, methotrexate, and cytarabine) replacement therapy. DEX (33 mg/day) was administered intravenously on days 1-4 and days 11-14 of R-HyperCVAD treatment, and aprepitant (APR) was administered on days 1-5 in both courses. The TAC C/D ratio decreased to approximately 1 on day 11 during both courses, and then increased. Furthermore, a decreasing trend in the TAC C/D ratio was observed after R-MA therapy. The decrease in the TAC C/D ratio was attributed to APR administration rather than to DEX.</p><p><strong>Conclusion: </strong>The induction of CYP3A activity by a high dose of DEX may not be strong. The pharmacokinetic information on DEX and in vitro enzyme activity induction studies also suggested that CYP3A activity induction is not prominent under high-dose DEX treatment.</p>","PeriodicalId":16730,"journal":{"name":"Journal of Pharmaceutical Health Care and Sciences","volume":"9 1","pages":"39"},"PeriodicalIF":1.3000,"publicationDate":"2023-12-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10694947/pdf/","citationCount":"0","resultStr":"{\"title\":\"Induction of CYP3A activity by dexamethasone may not be strong, even at high doses: insights from a case of tacrolimus co-administration.\",\"authors\":\"Yoshiyuki Ohno, Toyohito Oriyama, Akira Honda, Mineo Kurokawa, Tappei Takada\",\"doi\":\"10.1186/s40780-023-00310-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Dexamethasone (DEX) induces CYP3A activity in a concentration-dependent manner. However, no study has examined changes in the blood concentration of CYP3A substrate drugs when DEX is administered at high doses. Herein, we present a case in which tacrolimus (TAC), a typical CYP3A substrate drug, was co-administered with a chemotherapy regimen that included high-dose DEX.</p><p><strong>Case presentation: </strong>A 71-year-old woman underwent liver transplantation for hepatocellular carcinoma 18 years prior to her inclusion in this case study. She was receiving TAC orally at 2 mg/day and had a stable trough blood concentration of approximately 4 ng/mL and a trough blood concentration/dose (C/D) ratio of approximately 2. The patient was diagnosed with post-transplant lymphoproliferative disease (histological type: Burkitt's lymphoma) after admission. Thereafter, the patient received cyclophosphamide-prednisolone (CP), followed by two courses of R-HyperCVAD (rituximab, cyclophosphamide, doxorubicin, vincristine, and DEX) and R-MA (rituximab, methotrexate, and cytarabine) replacement therapy. DEX (33 mg/day) was administered intravenously on days 1-4 and days 11-14 of R-HyperCVAD treatment, and aprepitant (APR) was administered on days 1-5 in both courses. The TAC C/D ratio decreased to approximately 1 on day 11 during both courses, and then increased. Furthermore, a decreasing trend in the TAC C/D ratio was observed after R-MA therapy. The decrease in the TAC C/D ratio was attributed to APR administration rather than to DEX.</p><p><strong>Conclusion: </strong>The induction of CYP3A activity by a high dose of DEX may not be strong. The pharmacokinetic information on DEX and in vitro enzyme activity induction studies also suggested that CYP3A activity induction is not prominent under high-dose DEX treatment.</p>\",\"PeriodicalId\":16730,\"journal\":{\"name\":\"Journal of Pharmaceutical Health Care and Sciences\",\"volume\":\"9 1\",\"pages\":\"39\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2023-12-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10694947/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Pharmaceutical Health Care and Sciences\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40780-023-00310-0\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Pharmaceutical Health Care and Sciences","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40780-023-00310-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Induction of CYP3A activity by dexamethasone may not be strong, even at high doses: insights from a case of tacrolimus co-administration.
Background: Dexamethasone (DEX) induces CYP3A activity in a concentration-dependent manner. However, no study has examined changes in the blood concentration of CYP3A substrate drugs when DEX is administered at high doses. Herein, we present a case in which tacrolimus (TAC), a typical CYP3A substrate drug, was co-administered with a chemotherapy regimen that included high-dose DEX.
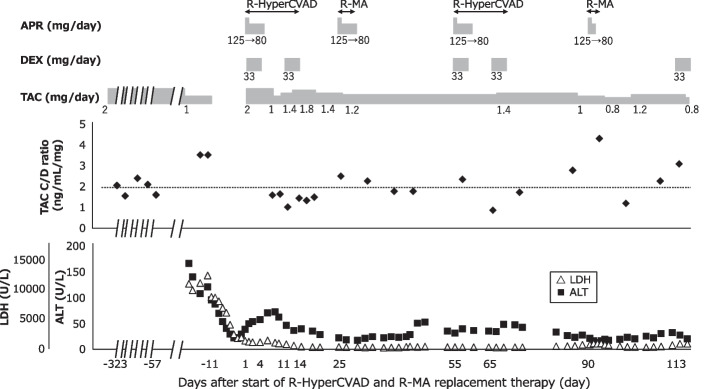
Case presentation: A 71-year-old woman underwent liver transplantation for hepatocellular carcinoma 18 years prior to her inclusion in this case study. She was receiving TAC orally at 2 mg/day and had a stable trough blood concentration of approximately 4 ng/mL and a trough blood concentration/dose (C/D) ratio of approximately 2. The patient was diagnosed with post-transplant lymphoproliferative disease (histological type: Burkitt's lymphoma) after admission. Thereafter, the patient received cyclophosphamide-prednisolone (CP), followed by two courses of R-HyperCVAD (rituximab, cyclophosphamide, doxorubicin, vincristine, and DEX) and R-MA (rituximab, methotrexate, and cytarabine) replacement therapy. DEX (33 mg/day) was administered intravenously on days 1-4 and days 11-14 of R-HyperCVAD treatment, and aprepitant (APR) was administered on days 1-5 in both courses. The TAC C/D ratio decreased to approximately 1 on day 11 during both courses, and then increased. Furthermore, a decreasing trend in the TAC C/D ratio was observed after R-MA therapy. The decrease in the TAC C/D ratio was attributed to APR administration rather than to DEX.
Conclusion: The induction of CYP3A activity by a high dose of DEX may not be strong. The pharmacokinetic information on DEX and in vitro enzyme activity induction studies also suggested that CYP3A activity induction is not prominent under high-dose DEX treatment.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
