{"title":"术后纵向疼痛数据缺失对腹部手术后第一天腹横肌平面阻滞镇痛研究结果的影响:单中心回顾性病历审查。","authors":"James Harvey Jones","doi":"10.2147/LRA.S439429","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The aims of this study are to analyze the association between the number of recorded pain scores and baseline pain following surgery, analgesia technique, and patient demographics, as well as the substitution of missing data with the results from mean substitution, last observation carried forward, regression imputation, multiple imputation, and mixed models.</p><p><strong>Methods: </strong>This retrospective chart review was approved by the Institutional Review Board (IRB). The following data were collected: patient demographics (age, gender, body mass index (BMI), race, and ethnicity); surgery type and date; analgesia with or without transversus abdominis plane (TAP) block; as well as the time, date, and value for all postoperative pain scores on the first postoperative day (POD). The following null hypotheses were tested: (1) the number of pain recordings will be independent of TAP block analgesia, baseline pain on POD 1, and patient demographics; and (2) there will be no significant differences in pain scores with and without TAP block analgesia following complete case analysis, mean substitution, last observation carried forward, regression imputation, multiple imputation, and mixed models.</p><p><strong>Results: </strong>This study analyzed 486 patients including 2562 recorded pain scores. An increase in age by one year is, on average, associated with a 0.04 (95% confidence interval (CI) -0.060 to -0.025) decrease in the number of pain scores recorded (p < 0.001). Black race is associated with 0.763 less pain scores, on average (95% CI -1.49 to -0.039) and this value is statistically significant (p = 0.039). All datasets with substituted values for missing data yield lower pain scores for patients who did not receive TAP block. Significant differences in recorded pain scores are only noted for scores recorded between 0400 and 0759 and 1600-1959 in mixed models.</p><p><strong>Conclusion: </strong>Discrepancies in pain score recordings among patients are associated with age and black race. When these discrepancies are addressed with statistical methods, clinically significant differences are appreciated.</p>","PeriodicalId":18203,"journal":{"name":"Local and Regional Anesthesia","volume":"16 ","pages":"173-182"},"PeriodicalIF":1.9000,"publicationDate":"2023-11-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10695121/pdf/","citationCount":"0","resultStr":"{\"title\":\"The Impact of Missing Postoperative Longitudinal Pain Data on Study Results Investigating Analgesia from Transversus Abdominis Plane Block on Postoperative Day One Following Abdominal Surgery: A Single-Center Retrospective Chart Review.\",\"authors\":\"James Harvey Jones\",\"doi\":\"10.2147/LRA.S439429\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The aims of this study are to analyze the association between the number of recorded pain scores and baseline pain following surgery, analgesia technique, and patient demographics, as well as the substitution of missing data with the results from mean substitution, last observation carried forward, regression imputation, multiple imputation, and mixed models.</p><p><strong>Methods: </strong>This retrospective chart review was approved by the Institutional Review Board (IRB). The following data were collected: patient demographics (age, gender, body mass index (BMI), race, and ethnicity); surgery type and date; analgesia with or without transversus abdominis plane (TAP) block; as well as the time, date, and value for all postoperative pain scores on the first postoperative day (POD). The following null hypotheses were tested: (1) the number of pain recordings will be independent of TAP block analgesia, baseline pain on POD 1, and patient demographics; and (2) there will be no significant differences in pain scores with and without TAP block analgesia following complete case analysis, mean substitution, last observation carried forward, regression imputation, multiple imputation, and mixed models.</p><p><strong>Results: </strong>This study analyzed 486 patients including 2562 recorded pain scores. An increase in age by one year is, on average, associated with a 0.04 (95% confidence interval (CI) -0.060 to -0.025) decrease in the number of pain scores recorded (p < 0.001). Black race is associated with 0.763 less pain scores, on average (95% CI -1.49 to -0.039) and this value is statistically significant (p = 0.039). All datasets with substituted values for missing data yield lower pain scores for patients who did not receive TAP block. Significant differences in recorded pain scores are only noted for scores recorded between 0400 and 0759 and 1600-1959 in mixed models.</p><p><strong>Conclusion: </strong>Discrepancies in pain score recordings among patients are associated with age and black race. When these discrepancies are addressed with statistical methods, clinically significant differences are appreciated.</p>\",\"PeriodicalId\":18203,\"journal\":{\"name\":\"Local and Regional Anesthesia\",\"volume\":\"16 \",\"pages\":\"173-182\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2023-11-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10695121/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Local and Regional Anesthesia\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/LRA.S439429\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Local and Regional Anesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/LRA.S439429","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
研究背景本研究的目的是分析记录的疼痛评分次数与术后基线疼痛、镇痛技术和患者人口统计学特征之间的关联,以及用平均替代、最后观察结转、回归归因、多重归因和混合模型的结果替代缺失数据:这项回顾性病历审查已获得机构审查委员会(IRB)批准。收集的数据包括:患者人口统计学特征(年龄、性别、体重指数 (BMI)、种族和民族);手术类型和日期;使用或不使用腹横肌平面 (TAP) 阻滞镇痛;以及术后第一天 (POD) 所有术后疼痛评分的时间、日期和数值。对以下零假设进行了检验:(1) 疼痛记录的数量与 TAP 阻滞镇痛、POD 1 的基线疼痛和患者人口统计学特征无关;(2) 经过完整病例分析、平均值替代、最后观察结果结转、回归归因、多重归因和混合模型分析后,采用 TAP 阻滞镇痛和未采用 TAP 阻滞镇痛的疼痛评分无显著差异:本研究分析了 486 名患者,包括 2562 份疼痛评分记录。年龄每增加一岁,记录的疼痛评分数量平均会减少 0.04(95% 置信区间 (CI) -0.060 至 -0.025)(p < 0.001)。黑种人的疼痛评分平均减少 0.763 分(95% CI -1.49 至 -0.039),且该值具有统计学意义(p = 0.039)。所有用替代值替代缺失数据的数据集都显示,未接受 TAP 阻滞的患者疼痛评分较低。在混合模型中,只有在 4:00 至 0759 和 16:00 至 1959 之间记录的疼痛评分存在显著差异:结论:患者疼痛评分记录的差异与年龄和黑人种族有关。结论:患者疼痛评分记录的差异与年龄和黑人种族有关。当使用统计方法处理这些差异时,就会发现有临床意义的差异。
The Impact of Missing Postoperative Longitudinal Pain Data on Study Results Investigating Analgesia from Transversus Abdominis Plane Block on Postoperative Day One Following Abdominal Surgery: A Single-Center Retrospective Chart Review.
Background: The aims of this study are to analyze the association between the number of recorded pain scores and baseline pain following surgery, analgesia technique, and patient demographics, as well as the substitution of missing data with the results from mean substitution, last observation carried forward, regression imputation, multiple imputation, and mixed models.
Methods: This retrospective chart review was approved by the Institutional Review Board (IRB). The following data were collected: patient demographics (age, gender, body mass index (BMI), race, and ethnicity); surgery type and date; analgesia with or without transversus abdominis plane (TAP) block; as well as the time, date, and value for all postoperative pain scores on the first postoperative day (POD). The following null hypotheses were tested: (1) the number of pain recordings will be independent of TAP block analgesia, baseline pain on POD 1, and patient demographics; and (2) there will be no significant differences in pain scores with and without TAP block analgesia following complete case analysis, mean substitution, last observation carried forward, regression imputation, multiple imputation, and mixed models.
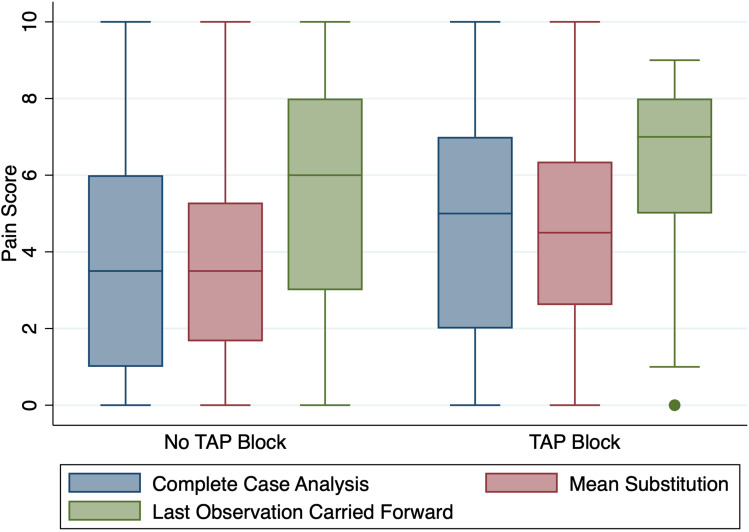
Results: This study analyzed 486 patients including 2562 recorded pain scores. An increase in age by one year is, on average, associated with a 0.04 (95% confidence interval (CI) -0.060 to -0.025) decrease in the number of pain scores recorded (p < 0.001). Black race is associated with 0.763 less pain scores, on average (95% CI -1.49 to -0.039) and this value is statistically significant (p = 0.039). All datasets with substituted values for missing data yield lower pain scores for patients who did not receive TAP block. Significant differences in recorded pain scores are only noted for scores recorded between 0400 and 0759 and 1600-1959 in mixed models.
Conclusion: Discrepancies in pain score recordings among patients are associated with age and black race. When these discrepancies are addressed with statistical methods, clinically significant differences are appreciated.






 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
