{"title":"如何预防癌症微创胃切除术后的严重腹腔内感染并发症?使用计算机断层扫描图像(脐-椎体最小直径)和机器人手术的新型标记的实用性","authors":"Naoshi Kubo, Katsunobu Sakurai, Tsuyoshi Hasegawa, Junya Nishimura, Yasuhito Iseki, Takafumi Nishii, Sadatoshi Shimizu, Toru Inoue, Yukio Nishiguchi, Kiyoshi Maeda","doi":"10.1002/ags3.12760","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Intra-abdominal infectious complications (IAICs) following minimally invasive gastrectomy (MIG) for cancer sometimes worsen short- and long-term outcomes. In this study, we focused on the minimum umbilicus–vertebra diameter (MUVD) in preoperative computed tomography (CT) images and robotic surgery to prevent severe IAIC occurrence.</p>\n </section>\n \n <section>\n \n <h3> Patients and Methods</h3>\n \n <p>A total of 400 patients with gastric cancer who underwent 204 laparoscopic gastrectomy (LG) and 196 robotic gastrectomy (RG) procedures were enrolled in this study. We retrospectively investigated the significance of the MUVD and robotic surgery for preventing severe IAICs following MIG using multivariate and propensity score matching analysis.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>The MUVD cutoff value was 84 mm by receiver operating characteristic (ROC) curve using severe IAICs as the end point. The MUVD and visceral fat area (VFA) had significantly higher area under the curve (AUC) than BMI (MUVD vs. BMI, <i>p</i> = 0.032; VFA vs. BMI, <i>p</i> < 0.01). In the multivariate analysis, high MUVD (HR, 9.46; <i>p</i> = 0.026) and laparoscopic surgery (HR, 3.35; <i>p</i> = 0.042) were independent risk factors for severe IAIC occurrence. In the propensity matching analysis between robotic and laparoscopic surgery in the high MUVD group, the RG group tended to have a lower severe IAIC rate than the LG group (0% vs. 9.8%, <i>p</i> = 0.056).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>The MUVD was a novel and easy-measuring predictor of severe IAICs following MIG. Robotic surgery should be considered first in patients with gastric cancer having an MUVD value of 84 mm or higher from the perspective of severe IAIC occurrence.</p>\n </section>\n </div>","PeriodicalId":8030,"journal":{"name":"Annals of Gastroenterological Surgery","volume":"8 3","pages":"420-430"},"PeriodicalIF":3.2000,"publicationDate":"2023-12-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ags3.12760","citationCount":"0","resultStr":"{\"title\":\"How do we prevent severe intra-abdominal infectious complications following minimally invasive gastrectomy for cancer? The usefulness of a novel marker using computed tomography images (minimum umbilicus–vertebra diameter) and robotic surgery\",\"authors\":\"Naoshi Kubo, Katsunobu Sakurai, Tsuyoshi Hasegawa, Junya Nishimura, Yasuhito Iseki, Takafumi Nishii, Sadatoshi Shimizu, Toru Inoue, Yukio Nishiguchi, Kiyoshi Maeda\",\"doi\":\"10.1002/ags3.12760\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Intra-abdominal infectious complications (IAICs) following minimally invasive gastrectomy (MIG) for cancer sometimes worsen short- and long-term outcomes. In this study, we focused on the minimum umbilicus–vertebra diameter (MUVD) in preoperative computed tomography (CT) images and robotic surgery to prevent severe IAIC occurrence.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Patients and Methods</h3>\\n \\n <p>A total of 400 patients with gastric cancer who underwent 204 laparoscopic gastrectomy (LG) and 196 robotic gastrectomy (RG) procedures were enrolled in this study. We retrospectively investigated the significance of the MUVD and robotic surgery for preventing severe IAICs following MIG using multivariate and propensity score matching analysis.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>The MUVD cutoff value was 84 mm by receiver operating characteristic (ROC) curve using severe IAICs as the end point. The MUVD and visceral fat area (VFA) had significantly higher area under the curve (AUC) than BMI (MUVD vs. BMI, <i>p</i> = 0.032; VFA vs. BMI, <i>p</i> < 0.01). In the multivariate analysis, high MUVD (HR, 9.46; <i>p</i> = 0.026) and laparoscopic surgery (HR, 3.35; <i>p</i> = 0.042) were independent risk factors for severe IAIC occurrence. In the propensity matching analysis between robotic and laparoscopic surgery in the high MUVD group, the RG group tended to have a lower severe IAIC rate than the LG group (0% vs. 9.8%, <i>p</i> = 0.056).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>The MUVD was a novel and easy-measuring predictor of severe IAICs following MIG. Robotic surgery should be considered first in patients with gastric cancer having an MUVD value of 84 mm or higher from the perspective of severe IAIC occurrence.</p>\\n </section>\\n </div>\",\"PeriodicalId\":8030,\"journal\":{\"name\":\"Annals of Gastroenterological Surgery\",\"volume\":\"8 3\",\"pages\":\"420-430\"},\"PeriodicalIF\":3.2000,\"publicationDate\":\"2023-12-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ags3.12760\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Gastroenterological Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ags3.12760\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Gastroenterological Surgery","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ags3.12760","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
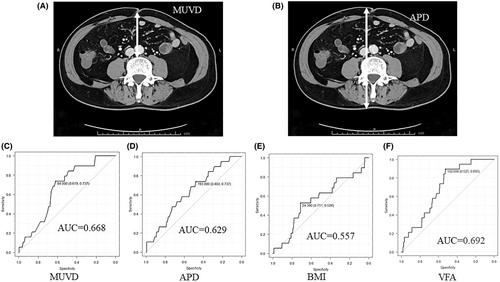
微创胃切除术(MIG)治疗癌症后腹腔内感染并发症(iiac)有时会恶化短期和长期预后。在本研究中,我们重点关注术前计算机断层扫描(CT)图像中的最小脐椎体直径(MUVD)和机器人手术,以防止严重的IAIC发生。共有400名胃癌患者接受了204例腹腔镜胃切除术(LG)和196例机器人胃切除术(RG)。我们采用多变量和倾向评分匹配分析回顾性研究了MUVD和机器人手术在预防MIG后严重iiac中的意义。以重度iiac为终点的受试者工作特征(ROC)曲线MUVD截止值为84 mm。MUVD和内脏脂肪面积(VFA)的曲线下面积(AUC)明显高于BMI (MUVD vs. BMI, p = 0.032;VFA vs. BMI, p < 0.01)。多因素分析中,高MUVD (HR, 9.46;p = 0.026)和腹腔镜手术(HR, 3.35;p = 0.042)是严重IAIC发生的独立危险因素。在高MUVD组机器人和腹腔镜手术的倾向匹配分析中,RG组倾向于比LG组有更低的严重IAIC发生率(0%比9.8%,p = 0.056)。MUVD是一种新颖且易于测量的MIG后严重iiac预测指标。从IAIC发生严重的角度来看,对于MUVD值≥84 mm的胃癌患者,应优先考虑机器人手术。
How do we prevent severe intra-abdominal infectious complications following minimally invasive gastrectomy for cancer? The usefulness of a novel marker using computed tomography images (minimum umbilicus–vertebra diameter) and robotic surgery
Background
Intra-abdominal infectious complications (IAICs) following minimally invasive gastrectomy (MIG) for cancer sometimes worsen short- and long-term outcomes. In this study, we focused on the minimum umbilicus–vertebra diameter (MUVD) in preoperative computed tomography (CT) images and robotic surgery to prevent severe IAIC occurrence.
Patients and Methods
A total of 400 patients with gastric cancer who underwent 204 laparoscopic gastrectomy (LG) and 196 robotic gastrectomy (RG) procedures were enrolled in this study. We retrospectively investigated the significance of the MUVD and robotic surgery for preventing severe IAICs following MIG using multivariate and propensity score matching analysis.
Results
The MUVD cutoff value was 84 mm by receiver operating characteristic (ROC) curve using severe IAICs as the end point. The MUVD and visceral fat area (VFA) had significantly higher area under the curve (AUC) than BMI (MUVD vs. BMI, p = 0.032; VFA vs. BMI, p < 0.01). In the multivariate analysis, high MUVD (HR, 9.46; p = 0.026) and laparoscopic surgery (HR, 3.35; p = 0.042) were independent risk factors for severe IAIC occurrence. In the propensity matching analysis between robotic and laparoscopic surgery in the high MUVD group, the RG group tended to have a lower severe IAIC rate than the LG group (0% vs. 9.8%, p = 0.056).
Conclusion
The MUVD was a novel and easy-measuring predictor of severe IAICs following MIG. Robotic surgery should be considered first in patients with gastric cancer having an MUVD value of 84 mm or higher from the perspective of severe IAIC occurrence.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
