Ismaheel O Lawal, Mehmet A Bilen, Raghuveer K Halkar, Ashesh B Jani, David M Schuster
{"title":"前列腺癌骨骼转移:无需治疗即可从溶骨形态自发演变为成骨形态。","authors":"Ismaheel O Lawal, Mehmet A Bilen, Raghuveer K Halkar, Ashesh B Jani, David M Schuster","doi":"10.1055/s-0043-1777697","DOIUrl":null,"url":null,"abstract":"<p><p>Skeletal metastases due to prostate cancer (PCa) are more commonly osteoblastic than osteolytic. In the rarer cases of osteolytic skeletal metastasis of PCa, transition to osteoblastic phenotype occurs following treatment, which indicates successful healing. In this report, we present a case of spontaneous osteolytic to osteoblastic evolution of PCa skeletal metastasis without treatment in a patient with recurrence of PCa. Our patient is a 59-year-old male who had a robotic radical prostatectomy in July 2014 for a T2c adenocarcinoma of the prostate gland (Gleason score = 4 + 3). He had adjuvant pelvic radiotherapy in January 2015 due to prostate-specific antigen (PSA) persistence. PSA began to rise in October 2015. An <sup>18</sup> F-fluciclovine positron emission tomography/computed tomography (PET/CT) scan obtained in June 2017 at a PSA of 0.5 ng/mL was negative. Repeat <sup>18</sup> F-fluciclovine PET/CT of February 2020 at PSA of 3.72 ng/mL showed prostate bed recurrence and a nonavid osteolytic left inferior pubic ramus lesion. 18F radiohybrid prostate-specific membrane antigen ( <sup>18</sup> F-rhPSMA) PET/CT scan of August 2020 performed as part of an ongoing clinical trial confirmed local prostate bed recurrence with a low-grade radiotracer uptake in the osteolytic left inferior pubic ramus bone lesion. Without salvage therapy, <sup>18</sup> F-fluciclovine PET/CT of October 2020 and March 2022 shows progressive sclerosis in the left pubic ramus lesion. An osteolytic to osteoblastic transition of a bone lesion as shown in this patient calls for a rethink in our understanding of untreated PCa skeletal metastasis progression. This case provides novel insight into the understanding of the temporal evolution of skeletal metastasis and calls for further research.</p>","PeriodicalId":23742,"journal":{"name":"World Journal of Nuclear Medicine","volume":"22 4","pages":"316-320"},"PeriodicalIF":1.0000,"publicationDate":"2023-12-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10751110/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prostate Cancer Skeletal Metastasis: A Spontaneous Evolution from Osteolytic to Osteoblastic Morphology without Treatment.\",\"authors\":\"Ismaheel O Lawal, Mehmet A Bilen, Raghuveer K Halkar, Ashesh B Jani, David M Schuster\",\"doi\":\"10.1055/s-0043-1777697\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Skeletal metastases due to prostate cancer (PCa) are more commonly osteoblastic than osteolytic. In the rarer cases of osteolytic skeletal metastasis of PCa, transition to osteoblastic phenotype occurs following treatment, which indicates successful healing. In this report, we present a case of spontaneous osteolytic to osteoblastic evolution of PCa skeletal metastasis without treatment in a patient with recurrence of PCa. Our patient is a 59-year-old male who had a robotic radical prostatectomy in July 2014 for a T2c adenocarcinoma of the prostate gland (Gleason score = 4 + 3). He had adjuvant pelvic radiotherapy in January 2015 due to prostate-specific antigen (PSA) persistence. PSA began to rise in October 2015. An <sup>18</sup> F-fluciclovine positron emission tomography/computed tomography (PET/CT) scan obtained in June 2017 at a PSA of 0.5 ng/mL was negative. Repeat <sup>18</sup> F-fluciclovine PET/CT of February 2020 at PSA of 3.72 ng/mL showed prostate bed recurrence and a nonavid osteolytic left inferior pubic ramus lesion. 18F radiohybrid prostate-specific membrane antigen ( <sup>18</sup> F-rhPSMA) PET/CT scan of August 2020 performed as part of an ongoing clinical trial confirmed local prostate bed recurrence with a low-grade radiotracer uptake in the osteolytic left inferior pubic ramus bone lesion. Without salvage therapy, <sup>18</sup> F-fluciclovine PET/CT of October 2020 and March 2022 shows progressive sclerosis in the left pubic ramus lesion. An osteolytic to osteoblastic transition of a bone lesion as shown in this patient calls for a rethink in our understanding of untreated PCa skeletal metastasis progression. This case provides novel insight into the understanding of the temporal evolution of skeletal metastasis and calls for further research.</p>\",\"PeriodicalId\":23742,\"journal\":{\"name\":\"World Journal of Nuclear Medicine\",\"volume\":\"22 4\",\"pages\":\"316-320\"},\"PeriodicalIF\":1.0000,\"publicationDate\":\"2023-12-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10751110/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Nuclear Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/s-0043-1777697\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/12/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Nuclear Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0043-1777697","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/12/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
Prostate Cancer Skeletal Metastasis: A Spontaneous Evolution from Osteolytic to Osteoblastic Morphology without Treatment.
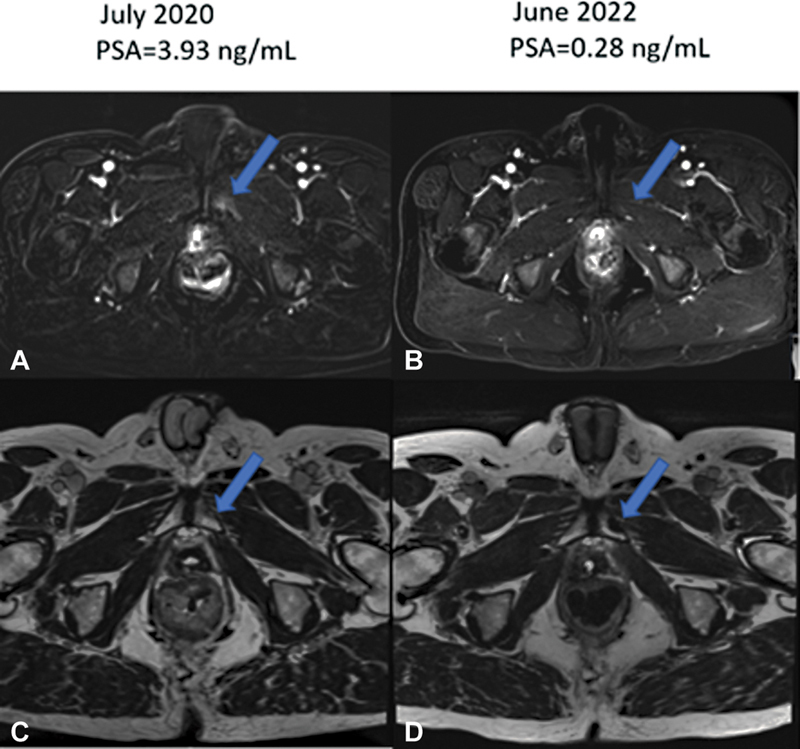
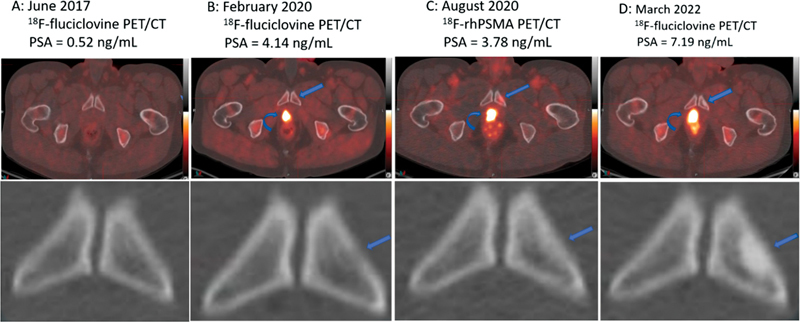
Skeletal metastases due to prostate cancer (PCa) are more commonly osteoblastic than osteolytic. In the rarer cases of osteolytic skeletal metastasis of PCa, transition to osteoblastic phenotype occurs following treatment, which indicates successful healing. In this report, we present a case of spontaneous osteolytic to osteoblastic evolution of PCa skeletal metastasis without treatment in a patient with recurrence of PCa. Our patient is a 59-year-old male who had a robotic radical prostatectomy in July 2014 for a T2c adenocarcinoma of the prostate gland (Gleason score = 4 + 3). He had adjuvant pelvic radiotherapy in January 2015 due to prostate-specific antigen (PSA) persistence. PSA began to rise in October 2015. An 18 F-fluciclovine positron emission tomography/computed tomography (PET/CT) scan obtained in June 2017 at a PSA of 0.5 ng/mL was negative. Repeat 18 F-fluciclovine PET/CT of February 2020 at PSA of 3.72 ng/mL showed prostate bed recurrence and a nonavid osteolytic left inferior pubic ramus lesion. 18F radiohybrid prostate-specific membrane antigen ( 18 F-rhPSMA) PET/CT scan of August 2020 performed as part of an ongoing clinical trial confirmed local prostate bed recurrence with a low-grade radiotracer uptake in the osteolytic left inferior pubic ramus bone lesion. Without salvage therapy, 18 F-fluciclovine PET/CT of October 2020 and March 2022 shows progressive sclerosis in the left pubic ramus lesion. An osteolytic to osteoblastic transition of a bone lesion as shown in this patient calls for a rethink in our understanding of untreated PCa skeletal metastasis progression. This case provides novel insight into the understanding of the temporal evolution of skeletal metastasis and calls for further research.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
