Lalit Takia, Arun K Baranwal, Pramod K Gupta, Muralidharan Jayashree, Suresh Kumar Angurana
{"title":"对于急性腹泻和严重脱水并伴有严重非离子间隙代谢性酸血症的儿童,额外碳酸氢盐输注是对世界卫生组织补液疗法的补充:一项开放标签随机试验。","authors":"Lalit Takia, Arun K Baranwal, Pramod K Gupta, Muralidharan Jayashree, Suresh Kumar Angurana","doi":"10.1007/s12098-023-04925-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To assess the efficacy and safety of bicarbonate infusion in children with Acute Diarrhea and Severe Dehydration (ADSD) having severe Non-Anion Gap Metabolic Acidemia (sNAGMA).</p><p><strong>Methods: </strong>Children (aged 1-144 mo) with ADSD and sNAGMA (pH ≤7.2 and/or serum bicarbonate ≤15 mEq/L) were enrolled in an open-label randomized design. Controls (n = 25) received WHO-recommended rehydration therapy with Ringer Lactate, while intervention group (n = 25) received additional bicarbonate deficit correction. Primary outcome was time taken to resolve metabolic acidemia (pH >7.30 and/or bicarbonate >15 mEq/L). Secondary outcome measures were adverse outcome [composite of pediatric intensive care unit (PICU) transfer and deaths], acute care area free days in 5 d (ACAFD<sub>5</sub>), hospital stay, and adverse effects.</p><p><strong>Results: </strong>Time taken to resolve metabolic acidemia was significantly lesser with intervention [median (IQR); 8 h (4, 12) vs. 12 h (8, 24); p = 0.0067]. Intervention led to acidemia resolution in significantly more children by 8 h and 16 h (17/25 vs. 9/25, p = 0.035 and 23/25 vs. 17/24, p = 0.018, respectively). Patients with fluid refractory shock needed lesser inotropes in intervention group [median Vasoactive Inotrope Score (VIS), 10.5 vs. 34]. Intervention led to significantly lesser adverse outcome (0/25 vs. 5/25, p = 0.049), and noticeably more ACAFD<sub>5</sub> [median (IQR); 2 (1, 2) vs. 1 (1, 2); p = 0.12]. Two patients died in the control group while none in the intervention group. No adverse effect was documented.</p><p><strong>Conclusions: </strong>Additional calculated dose of bicarbonate infusion led to significantly early resolution of metabolic acidemia, lesser utilization of critical care facilities, and lesser adverse outcome in children with ADSD and sNAGMA, compared to standard therapy, with no adverse effect.</p>","PeriodicalId":13320,"journal":{"name":"Indian Journal of Pediatrics","volume":" ","pages":"268-276"},"PeriodicalIF":2.1000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Additional Bicarbonate Infusion Complements WHO Rehydration Therapy in Children with Acute Diarrhea and Severe Dehydration Presenting with Severe Non-anion Gap Metabolic Acidemia: An Open Label Randomized Trial.\",\"authors\":\"Lalit Takia, Arun K Baranwal, Pramod K Gupta, Muralidharan Jayashree, Suresh Kumar Angurana\",\"doi\":\"10.1007/s12098-023-04925-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To assess the efficacy and safety of bicarbonate infusion in children with Acute Diarrhea and Severe Dehydration (ADSD) having severe Non-Anion Gap Metabolic Acidemia (sNAGMA).</p><p><strong>Methods: </strong>Children (aged 1-144 mo) with ADSD and sNAGMA (pH ≤7.2 and/or serum bicarbonate ≤15 mEq/L) were enrolled in an open-label randomized design. Controls (n = 25) received WHO-recommended rehydration therapy with Ringer Lactate, while intervention group (n = 25) received additional bicarbonate deficit correction. Primary outcome was time taken to resolve metabolic acidemia (pH >7.30 and/or bicarbonate >15 mEq/L). Secondary outcome measures were adverse outcome [composite of pediatric intensive care unit (PICU) transfer and deaths], acute care area free days in 5 d (ACAFD<sub>5</sub>), hospital stay, and adverse effects.</p><p><strong>Results: </strong>Time taken to resolve metabolic acidemia was significantly lesser with intervention [median (IQR); 8 h (4, 12) vs. 12 h (8, 24); p = 0.0067]. Intervention led to acidemia resolution in significantly more children by 8 h and 16 h (17/25 vs. 9/25, p = 0.035 and 23/25 vs. 17/24, p = 0.018, respectively). Patients with fluid refractory shock needed lesser inotropes in intervention group [median Vasoactive Inotrope Score (VIS), 10.5 vs. 34]. Intervention led to significantly lesser adverse outcome (0/25 vs. 5/25, p = 0.049), and noticeably more ACAFD<sub>5</sub> [median (IQR); 2 (1, 2) vs. 1 (1, 2); p = 0.12]. Two patients died in the control group while none in the intervention group. No adverse effect was documented.</p><p><strong>Conclusions: </strong>Additional calculated dose of bicarbonate infusion led to significantly early resolution of metabolic acidemia, lesser utilization of critical care facilities, and lesser adverse outcome in children with ADSD and sNAGMA, compared to standard therapy, with no adverse effect.</p>\",\"PeriodicalId\":13320,\"journal\":{\"name\":\"Indian Journal of Pediatrics\",\"volume\":\" \",\"pages\":\"268-276\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2025-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Indian Journal of Pediatrics\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s12098-023-04925-x\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/12/29 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Indian Journal of Pediatrics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s12098-023-04925-x","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/12/29 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
Additional Bicarbonate Infusion Complements WHO Rehydration Therapy in Children with Acute Diarrhea and Severe Dehydration Presenting with Severe Non-anion Gap Metabolic Acidemia: An Open Label Randomized Trial.
Objectives: To assess the efficacy and safety of bicarbonate infusion in children with Acute Diarrhea and Severe Dehydration (ADSD) having severe Non-Anion Gap Metabolic Acidemia (sNAGMA).
Methods: Children (aged 1-144 mo) with ADSD and sNAGMA (pH ≤7.2 and/or serum bicarbonate ≤15 mEq/L) were enrolled in an open-label randomized design. Controls (n = 25) received WHO-recommended rehydration therapy with Ringer Lactate, while intervention group (n = 25) received additional bicarbonate deficit correction. Primary outcome was time taken to resolve metabolic acidemia (pH >7.30 and/or bicarbonate >15 mEq/L). Secondary outcome measures were adverse outcome [composite of pediatric intensive care unit (PICU) transfer and deaths], acute care area free days in 5 d (ACAFD5), hospital stay, and adverse effects.
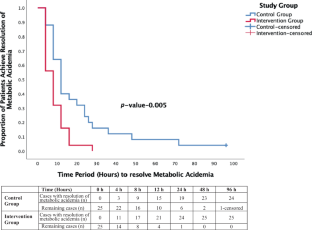
Results: Time taken to resolve metabolic acidemia was significantly lesser with intervention [median (IQR); 8 h (4, 12) vs. 12 h (8, 24); p = 0.0067]. Intervention led to acidemia resolution in significantly more children by 8 h and 16 h (17/25 vs. 9/25, p = 0.035 and 23/25 vs. 17/24, p = 0.018, respectively). Patients with fluid refractory shock needed lesser inotropes in intervention group [median Vasoactive Inotrope Score (VIS), 10.5 vs. 34]. Intervention led to significantly lesser adverse outcome (0/25 vs. 5/25, p = 0.049), and noticeably more ACAFD5 [median (IQR); 2 (1, 2) vs. 1 (1, 2); p = 0.12]. Two patients died in the control group while none in the intervention group. No adverse effect was documented.
Conclusions: Additional calculated dose of bicarbonate infusion led to significantly early resolution of metabolic acidemia, lesser utilization of critical care facilities, and lesser adverse outcome in children with ADSD and sNAGMA, compared to standard therapy, with no adverse effect.
期刊介绍:
Indian Journal of Pediatrics (IJP), is an official publication of the Dr. K.C. Chaudhuri Foundation. The Journal, a peer-reviewed publication, is published twelve times a year on a monthly basis (January, February, March, April, May, June, July, August, September, October, November, December), and publishes clinical and basic research of all aspects of pediatrics, provided they have scientific merit and represent an important advance in knowledge. The Journal publishes original articles, review articles, case reports which provide new information, letters in relation to published articles, scientific research letters and picture of the month, announcements (meetings, courses, job advertisements); summary report of conferences and book reviews.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
