Louisa P. Selvadurai, Susan L. Perlman, Tetsuo Ashizawa, George R. Wilmot, Chiadi U. Onyike, Liana S. Rosenthal, Vikram G. Shakkottai, Henry L. Paulson, Sub H. Subramony, Khalaf O. Bushara, Sheng-Han Kuo, Cameron Dietiker, Michael D. Geschwind, Alexandra B. Nelson, Christopher M. Gomez, Puneet Opal, Theresa A. Zesiewicz, Trevor Hawkins, Talene A. Yacoubian, Peggy C. Nopoulos, Sharon J. Sha, Peter E. Morrison, Karla P. Figueroa, Stefan M. Pulst, Jeremy D. Schmahmann
{"title":"脊髓小脑性共济失调的小脑认知情感/施马曼综合征量表","authors":"Louisa P. Selvadurai, Susan L. Perlman, Tetsuo Ashizawa, George R. Wilmot, Chiadi U. Onyike, Liana S. Rosenthal, Vikram G. Shakkottai, Henry L. Paulson, Sub H. Subramony, Khalaf O. Bushara, Sheng-Han Kuo, Cameron Dietiker, Michael D. Geschwind, Alexandra B. Nelson, Christopher M. Gomez, Puneet Opal, Theresa A. Zesiewicz, Trevor Hawkins, Talene A. Yacoubian, Peggy C. Nopoulos, Sharon J. Sha, Peter E. Morrison, Karla P. Figueroa, Stefan M. Pulst, Jeremy D. Schmahmann","doi":"10.1007/s12311-023-01651-0","DOIUrl":null,"url":null,"abstract":"<p>The Cerebellar Cognitive Affective/Schmahmann Syndrome (CCAS) manifests as impaired executive control, linguistic processing, visual spatial function, and affect regulation. The CCAS has been described in the spinocerebellar ataxias (SCAs), but its prevalence is unknown. We analyzed results of the CCAS/Schmahmann Scale (CCAS-S), developed to detect and quantify CCAS, in two natural history studies of 309 individuals Symptomatic for SCA1, SCA2, SCA3, SCA6, SCA7, or SCA8, 26 individuals Pre-symptomatic for SCA1 or SCA3, and 37 Controls. We compared total raw scores, domain scores, and total fail scores between Symptomatic, Pre-symptomatic, and Control cohorts, and between SCA types. We calculated scale sensitivity and selectivity based on CCAS category designation among Symptomatic individuals and Controls, and correlated CCAS-S performance against age and education, and in Symptomatic patients, against genetic repeat length, onset age, disease duration, motor ataxia, depression, and fatigue. Definite CCAS was identified in 46% of the Symptomatic group. False positive rate among Controls was 5.4%. Symptomatic individuals had poorer global CCAS-S performance than Controls, accounting for age and education. The domains of semantic fluency, phonemic fluency, and category switching that tap executive function and linguistic processing consistently separated Symptomatic individuals from Controls. CCAS-S scores correlated most closely with motor ataxia. Controls were similar to Pre-symptomatic individuals whose nearness to symptom onset was unknown. The use of the CCAS-S identifies a high CCAS prevalence in a large cohort of SCA patients, underscoring the utility of the scale and the notion that the CCAS is the third cornerstone of clinical ataxiology.</p>","PeriodicalId":22415,"journal":{"name":"The Cerebellum","volume":"196 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2024-01-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"The Cerebellar Cognitive Affective/Schmahmann Syndrome Scale in Spinocerebellar Ataxias\",\"authors\":\"Louisa P. Selvadurai, Susan L. Perlman, Tetsuo Ashizawa, George R. Wilmot, Chiadi U. Onyike, Liana S. Rosenthal, Vikram G. Shakkottai, Henry L. Paulson, Sub H. Subramony, Khalaf O. Bushara, Sheng-Han Kuo, Cameron Dietiker, Michael D. Geschwind, Alexandra B. Nelson, Christopher M. Gomez, Puneet Opal, Theresa A. Zesiewicz, Trevor Hawkins, Talene A. Yacoubian, Peggy C. Nopoulos, Sharon J. Sha, Peter E. Morrison, Karla P. Figueroa, Stefan M. Pulst, Jeremy D. Schmahmann\",\"doi\":\"10.1007/s12311-023-01651-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>The Cerebellar Cognitive Affective/Schmahmann Syndrome (CCAS) manifests as impaired executive control, linguistic processing, visual spatial function, and affect regulation. The CCAS has been described in the spinocerebellar ataxias (SCAs), but its prevalence is unknown. We analyzed results of the CCAS/Schmahmann Scale (CCAS-S), developed to detect and quantify CCAS, in two natural history studies of 309 individuals Symptomatic for SCA1, SCA2, SCA3, SCA6, SCA7, or SCA8, 26 individuals Pre-symptomatic for SCA1 or SCA3, and 37 Controls. We compared total raw scores, domain scores, and total fail scores between Symptomatic, Pre-symptomatic, and Control cohorts, and between SCA types. We calculated scale sensitivity and selectivity based on CCAS category designation among Symptomatic individuals and Controls, and correlated CCAS-S performance against age and education, and in Symptomatic patients, against genetic repeat length, onset age, disease duration, motor ataxia, depression, and fatigue. Definite CCAS was identified in 46% of the Symptomatic group. False positive rate among Controls was 5.4%. Symptomatic individuals had poorer global CCAS-S performance than Controls, accounting for age and education. The domains of semantic fluency, phonemic fluency, and category switching that tap executive function and linguistic processing consistently separated Symptomatic individuals from Controls. CCAS-S scores correlated most closely with motor ataxia. Controls were similar to Pre-symptomatic individuals whose nearness to symptom onset was unknown. The use of the CCAS-S identifies a high CCAS prevalence in a large cohort of SCA patients, underscoring the utility of the scale and the notion that the CCAS is the third cornerstone of clinical ataxiology.</p>\",\"PeriodicalId\":22415,\"journal\":{\"name\":\"The Cerebellum\",\"volume\":\"196 1\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-01-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The Cerebellum\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s12311-023-01651-0\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Cerebellum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s12311-023-01651-0","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
The Cerebellar Cognitive Affective/Schmahmann Syndrome Scale in Spinocerebellar Ataxias
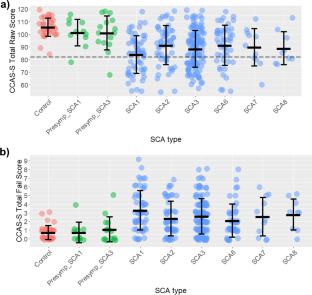
The Cerebellar Cognitive Affective/Schmahmann Syndrome (CCAS) manifests as impaired executive control, linguistic processing, visual spatial function, and affect regulation. The CCAS has been described in the spinocerebellar ataxias (SCAs), but its prevalence is unknown. We analyzed results of the CCAS/Schmahmann Scale (CCAS-S), developed to detect and quantify CCAS, in two natural history studies of 309 individuals Symptomatic for SCA1, SCA2, SCA3, SCA6, SCA7, or SCA8, 26 individuals Pre-symptomatic for SCA1 or SCA3, and 37 Controls. We compared total raw scores, domain scores, and total fail scores between Symptomatic, Pre-symptomatic, and Control cohorts, and between SCA types. We calculated scale sensitivity and selectivity based on CCAS category designation among Symptomatic individuals and Controls, and correlated CCAS-S performance against age and education, and in Symptomatic patients, against genetic repeat length, onset age, disease duration, motor ataxia, depression, and fatigue. Definite CCAS was identified in 46% of the Symptomatic group. False positive rate among Controls was 5.4%. Symptomatic individuals had poorer global CCAS-S performance than Controls, accounting for age and education. The domains of semantic fluency, phonemic fluency, and category switching that tap executive function and linguistic processing consistently separated Symptomatic individuals from Controls. CCAS-S scores correlated most closely with motor ataxia. Controls were similar to Pre-symptomatic individuals whose nearness to symptom onset was unknown. The use of the CCAS-S identifies a high CCAS prevalence in a large cohort of SCA patients, underscoring the utility of the scale and the notion that the CCAS is the third cornerstone of clinical ataxiology.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
