Gretchen Bjornstad, Shreya Sonthalia, Benjamin Rouse, Leanne Freeman, Natasha Hessami, Jo Hickman Dunne, Nick Axford
{"title":"基于交付特征的认知行为干预对青少年抑郁症状升高的有效性比较:系统综述","authors":"Gretchen Bjornstad, Shreya Sonthalia, Benjamin Rouse, Leanne Freeman, Natasha Hessami, Jo Hickman Dunne, Nick Axford","doi":"10.1002/cl2.1376","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Depression is a public health problem and common amongst adolescents. Cognitive behavioural therapy (CBT) is widely used to treat adolescent depression but existing research does not provide clear conclusions regarding the relative effectiveness of different delivery modalities.</p>\n </section>\n \n <section>\n \n <h3> Objectives</h3>\n \n <p>The primary aim is to estimate the relative efficacy of different modes of CBT delivery compared with each other and control conditions for reducing depressive symptoms in adolescents. The secondary aim is to compare the different modes of delivery with regard to intervention completion/attrition (a proxy for intervention acceptability).</p>\n </section>\n \n <section>\n \n <h3> Search Methods</h3>\n \n <p>The Cochrane Depression, Anxiety and Neurosis Clinical Trials Register was searched in April 2020. MEDLINE, PsycInfo, EMBASE, four other electronic databases, the CENTRAL trial registry, Google Scholar and Google were searched in November 2020, together with reference checking, citation searching and hand-searching of two databases.</p>\n </section>\n \n <section>\n \n <h3> Selection Criteria</h3>\n \n <p>Randomised controlled trials (RCTs) of CBT interventions (irrespective of delivery mode) to reduce symptoms of depression in young people aged 10–19 years with clinically relevant symptoms or diagnosis of depression were included.</p>\n </section>\n \n <section>\n \n <h3> Data Collection and Analysis</h3>\n \n <p>Screening and data extraction were completed by two authors independently, with discrepancies addressed by a third author. CBT interventions were categorised as follows: group CBT, individual CBT, remote CBT, guided self-help, and unguided self-help. Effect on depressive symptom score was estimated across validated self-report measures using Hedges' <i>g</i> standardised mean difference. Acceptability was estimated based on loss to follow-up as an odds ratio. Treatment rankings were developed using the surface under the cumulative ranking curve (SUCRA). Pairwise meta-analyses were conducted using random effects models where there were two or more head-to-head trials. Network analyses were conducted using random effects models.</p>\n </section>\n \n <section>\n \n <h3> Main Results</h3>\n \n <p>Sixty-eight studies were included in the review. The mean age of participants ranged from 10 to 19.5 years, and on average 60% of participants were female. The majority of studies were conducted in schools (28) or universities (6); other settings included primary care, clinical settings and the home. The number of CBT sessions ranged from 1 to 16, the frequency of delivery from once every 2 weeks to twice a week and the duration of each session from 20 min to 2 h. The risk of bias was low across all domains for 23 studies, 24 studies had some concerns and the remaining 21 were assessed to be at high risk of bias. Sixty-two RCTs (representing 6435 participants) were included in the pairwise and network meta-analyses for post-intervention depressive symptom score at post-intervention. All pre-specified treatment and control categories were represented by at least one RCT. Although most CBT approaches, except remote CBT, demonstrated superiority over no intervention, no approaches performed clearly better than or equivalent to another. The highest and lowest ranking interventions were guided self-help (SUCRA 83%) and unguided self-help (SUCRA 51%), respectively (very low certainty in treatment ranking). Nineteen RCTs (3260 participants) were included in the pairwise and network meta-analyses for 6 to 12 month follow-up depressive symptom score. Neither guided self-help nor remote CBT were evaluated in the RCTs for this time point. Effects were generally attenuated for 6- to 12-month outcomes compared to posttest. No interventions demonstrated superiority to no intervention, although unguided self-help and group CBT both demonstrated superiority compared to TAU. No CBT approach demonstrated clear superiority over another. The highest and lowest ranking approaches were unguided self-help and individual CBT, respectively. Sixty-two RCTs (7347 participants) were included in the pairwise and network meta-analyses for intervention acceptability. All pre-specified treatment and control categories were represented by at least one RCT. Although point estimates tended to favour no intervention, no active treatments were clearly inferior. No CBT approach demonstrated clear superiority over another. The highest and lowest ranking active interventions were individual CBT and group CBT respectively. Pairwise meta-analytic findings were similar to those of the network meta-analysis for all analyses. There may be age-based subgroup effects on post-intervention depressive symptoms. Using the no intervention control group as the reference, the magnitudes of effects appear to be larger for the oldest age categories compared to the other subgroups for each given comparison. However, they were generally less precise and formal testing only indicated a significant difference for group CBT. Findings were robust to pre-specified sensitivity analyses separating out the type of placebo and excluding cluster-RCTs, as well as an additional analysis excluding studies where we had imputed standard deviations.</p>\n </section>\n \n <section>\n \n <h3> Authors' Conclusions</h3>\n \n <p>At posttreatment, all active treatments (group CBT, individual CBT, guided self-help, and unguided self-help) except for remote CBT were more effective than no treatment. Guided self-help was the most highly ranked intervention but only evaluated in trials with the oldest adolescents (16–19 years). Moreover, the studies of guided self-help vary in the type and amount of therapist support provided and longer-term results are needed to determine whether effects persist. The magnitude of effects was generally attenuated for 6- to 12-month outcomes. Although unguided self-help was the lowest-ranked active intervention at post-intervention, it was the highest ranked at follow-up. This suggests the need for further research into whether interventions with self-directed elements enable young people to maintain effects by continuing or revisiting the intervention independently, and whether therapist support would improve long-term outcomes. There was no clear evidence that any active treatments were more acceptable to participants than any others. The relative effectiveness of intervention delivery modes must be taken into account in the context of the needs and preferences of individual young people, particularly as the differences between effect sizes were relatively small. Further research into the type and amount of therapist support that is most acceptable to young people and most cost-effective would be particularly useful.</p>\n </section>\n </div>","PeriodicalId":36698,"journal":{"name":"Campbell Systematic Reviews","volume":"20 1","pages":""},"PeriodicalIF":3.8000,"publicationDate":"2024-01-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cl2.1376","citationCount":"0","resultStr":"{\"title\":\"A comparison of the effectiveness of cognitive behavioural interventions based on delivery features for elevated symptoms of depression in adolescents: A systematic review\",\"authors\":\"Gretchen Bjornstad, Shreya Sonthalia, Benjamin Rouse, Leanne Freeman, Natasha Hessami, Jo Hickman Dunne, Nick Axford\",\"doi\":\"10.1002/cl2.1376\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Depression is a public health problem and common amongst adolescents. Cognitive behavioural therapy (CBT) is widely used to treat adolescent depression but existing research does not provide clear conclusions regarding the relative effectiveness of different delivery modalities.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Objectives</h3>\\n \\n <p>The primary aim is to estimate the relative efficacy of different modes of CBT delivery compared with each other and control conditions for reducing depressive symptoms in adolescents. The secondary aim is to compare the different modes of delivery with regard to intervention completion/attrition (a proxy for intervention acceptability).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Search Methods</h3>\\n \\n <p>The Cochrane Depression, Anxiety and Neurosis Clinical Trials Register was searched in April 2020. MEDLINE, PsycInfo, EMBASE, four other electronic databases, the CENTRAL trial registry, Google Scholar and Google were searched in November 2020, together with reference checking, citation searching and hand-searching of two databases.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Selection Criteria</h3>\\n \\n <p>Randomised controlled trials (RCTs) of CBT interventions (irrespective of delivery mode) to reduce symptoms of depression in young people aged 10–19 years with clinically relevant symptoms or diagnosis of depression were included.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Data Collection and Analysis</h3>\\n \\n <p>Screening and data extraction were completed by two authors independently, with discrepancies addressed by a third author. CBT interventions were categorised as follows: group CBT, individual CBT, remote CBT, guided self-help, and unguided self-help. Effect on depressive symptom score was estimated across validated self-report measures using Hedges' <i>g</i> standardised mean difference. Acceptability was estimated based on loss to follow-up as an odds ratio. Treatment rankings were developed using the surface under the cumulative ranking curve (SUCRA). Pairwise meta-analyses were conducted using random effects models where there were two or more head-to-head trials. Network analyses were conducted using random effects models.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Main Results</h3>\\n \\n <p>Sixty-eight studies were included in the review. The mean age of participants ranged from 10 to 19.5 years, and on average 60% of participants were female. The majority of studies were conducted in schools (28) or universities (6); other settings included primary care, clinical settings and the home. The number of CBT sessions ranged from 1 to 16, the frequency of delivery from once every 2 weeks to twice a week and the duration of each session from 20 min to 2 h. The risk of bias was low across all domains for 23 studies, 24 studies had some concerns and the remaining 21 were assessed to be at high risk of bias. Sixty-two RCTs (representing 6435 participants) were included in the pairwise and network meta-analyses for post-intervention depressive symptom score at post-intervention. All pre-specified treatment and control categories were represented by at least one RCT. Although most CBT approaches, except remote CBT, demonstrated superiority over no intervention, no approaches performed clearly better than or equivalent to another. The highest and lowest ranking interventions were guided self-help (SUCRA 83%) and unguided self-help (SUCRA 51%), respectively (very low certainty in treatment ranking). Nineteen RCTs (3260 participants) were included in the pairwise and network meta-analyses for 6 to 12 month follow-up depressive symptom score. Neither guided self-help nor remote CBT were evaluated in the RCTs for this time point. Effects were generally attenuated for 6- to 12-month outcomes compared to posttest. No interventions demonstrated superiority to no intervention, although unguided self-help and group CBT both demonstrated superiority compared to TAU. No CBT approach demonstrated clear superiority over another. The highest and lowest ranking approaches were unguided self-help and individual CBT, respectively. Sixty-two RCTs (7347 participants) were included in the pairwise and network meta-analyses for intervention acceptability. All pre-specified treatment and control categories were represented by at least one RCT. Although point estimates tended to favour no intervention, no active treatments were clearly inferior. No CBT approach demonstrated clear superiority over another. The highest and lowest ranking active interventions were individual CBT and group CBT respectively. Pairwise meta-analytic findings were similar to those of the network meta-analysis for all analyses. There may be age-based subgroup effects on post-intervention depressive symptoms. Using the no intervention control group as the reference, the magnitudes of effects appear to be larger for the oldest age categories compared to the other subgroups for each given comparison. However, they were generally less precise and formal testing only indicated a significant difference for group CBT. Findings were robust to pre-specified sensitivity analyses separating out the type of placebo and excluding cluster-RCTs, as well as an additional analysis excluding studies where we had imputed standard deviations.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Authors' Conclusions</h3>\\n \\n <p>At posttreatment, all active treatments (group CBT, individual CBT, guided self-help, and unguided self-help) except for remote CBT were more effective than no treatment. Guided self-help was the most highly ranked intervention but only evaluated in trials with the oldest adolescents (16–19 years). Moreover, the studies of guided self-help vary in the type and amount of therapist support provided and longer-term results are needed to determine whether effects persist. The magnitude of effects was generally attenuated for 6- to 12-month outcomes. Although unguided self-help was the lowest-ranked active intervention at post-intervention, it was the highest ranked at follow-up. This suggests the need for further research into whether interventions with self-directed elements enable young people to maintain effects by continuing or revisiting the intervention independently, and whether therapist support would improve long-term outcomes. There was no clear evidence that any active treatments were more acceptable to participants than any others. The relative effectiveness of intervention delivery modes must be taken into account in the context of the needs and preferences of individual young people, particularly as the differences between effect sizes were relatively small. Further research into the type and amount of therapist support that is most acceptable to young people and most cost-effective would be particularly useful.</p>\\n </section>\\n </div>\",\"PeriodicalId\":36698,\"journal\":{\"name\":\"Campbell Systematic Reviews\",\"volume\":\"20 1\",\"pages\":\"\"},\"PeriodicalIF\":3.8000,\"publicationDate\":\"2024-01-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cl2.1376\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Campbell Systematic Reviews\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/cl2.1376\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"SOCIAL SCIENCES, INTERDISCIPLINARY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Campbell Systematic Reviews","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cl2.1376","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SOCIAL SCIENCES, INTERDISCIPLINARY","Score":null,"Total":0}
A comparison of the effectiveness of cognitive behavioural interventions based on delivery features for elevated symptoms of depression in adolescents: A systematic review
Background
Depression is a public health problem and common amongst adolescents. Cognitive behavioural therapy (CBT) is widely used to treat adolescent depression but existing research does not provide clear conclusions regarding the relative effectiveness of different delivery modalities.
Objectives
The primary aim is to estimate the relative efficacy of different modes of CBT delivery compared with each other and control conditions for reducing depressive symptoms in adolescents. The secondary aim is to compare the different modes of delivery with regard to intervention completion/attrition (a proxy for intervention acceptability).
Search Methods
The Cochrane Depression, Anxiety and Neurosis Clinical Trials Register was searched in April 2020. MEDLINE, PsycInfo, EMBASE, four other electronic databases, the CENTRAL trial registry, Google Scholar and Google were searched in November 2020, together with reference checking, citation searching and hand-searching of two databases.
Selection Criteria
Randomised controlled trials (RCTs) of CBT interventions (irrespective of delivery mode) to reduce symptoms of depression in young people aged 10–19 years with clinically relevant symptoms or diagnosis of depression were included.
Data Collection and Analysis
Screening and data extraction were completed by two authors independently, with discrepancies addressed by a third author. CBT interventions were categorised as follows: group CBT, individual CBT, remote CBT, guided self-help, and unguided self-help. Effect on depressive symptom score was estimated across validated self-report measures using Hedges' g standardised mean difference. Acceptability was estimated based on loss to follow-up as an odds ratio. Treatment rankings were developed using the surface under the cumulative ranking curve (SUCRA). Pairwise meta-analyses were conducted using random effects models where there were two or more head-to-head trials. Network analyses were conducted using random effects models.
Main Results
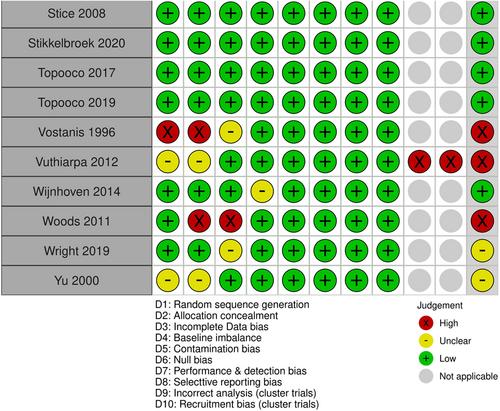
Sixty-eight studies were included in the review. The mean age of participants ranged from 10 to 19.5 years, and on average 60% of participants were female. The majority of studies were conducted in schools (28) or universities (6); other settings included primary care, clinical settings and the home. The number of CBT sessions ranged from 1 to 16, the frequency of delivery from once every 2 weeks to twice a week and the duration of each session from 20 min to 2 h. The risk of bias was low across all domains for 23 studies, 24 studies had some concerns and the remaining 21 were assessed to be at high risk of bias. Sixty-two RCTs (representing 6435 participants) were included in the pairwise and network meta-analyses for post-intervention depressive symptom score at post-intervention. All pre-specified treatment and control categories were represented by at least one RCT. Although most CBT approaches, except remote CBT, demonstrated superiority over no intervention, no approaches performed clearly better than or equivalent to another. The highest and lowest ranking interventions were guided self-help (SUCRA 83%) and unguided self-help (SUCRA 51%), respectively (very low certainty in treatment ranking). Nineteen RCTs (3260 participants) were included in the pairwise and network meta-analyses for 6 to 12 month follow-up depressive symptom score. Neither guided self-help nor remote CBT were evaluated in the RCTs for this time point. Effects were generally attenuated for 6- to 12-month outcomes compared to posttest. No interventions demonstrated superiority to no intervention, although unguided self-help and group CBT both demonstrated superiority compared to TAU. No CBT approach demonstrated clear superiority over another. The highest and lowest ranking approaches were unguided self-help and individual CBT, respectively. Sixty-two RCTs (7347 participants) were included in the pairwise and network meta-analyses for intervention acceptability. All pre-specified treatment and control categories were represented by at least one RCT. Although point estimates tended to favour no intervention, no active treatments were clearly inferior. No CBT approach demonstrated clear superiority over another. The highest and lowest ranking active interventions were individual CBT and group CBT respectively. Pairwise meta-analytic findings were similar to those of the network meta-analysis for all analyses. There may be age-based subgroup effects on post-intervention depressive symptoms. Using the no intervention control group as the reference, the magnitudes of effects appear to be larger for the oldest age categories compared to the other subgroups for each given comparison. However, they were generally less precise and formal testing only indicated a significant difference for group CBT. Findings were robust to pre-specified sensitivity analyses separating out the type of placebo and excluding cluster-RCTs, as well as an additional analysis excluding studies where we had imputed standard deviations.
Authors' Conclusions
At posttreatment, all active treatments (group CBT, individual CBT, guided self-help, and unguided self-help) except for remote CBT were more effective than no treatment. Guided self-help was the most highly ranked intervention but only evaluated in trials with the oldest adolescents (16–19 years). Moreover, the studies of guided self-help vary in the type and amount of therapist support provided and longer-term results are needed to determine whether effects persist. The magnitude of effects was generally attenuated for 6- to 12-month outcomes. Although unguided self-help was the lowest-ranked active intervention at post-intervention, it was the highest ranked at follow-up. This suggests the need for further research into whether interventions with self-directed elements enable young people to maintain effects by continuing or revisiting the intervention independently, and whether therapist support would improve long-term outcomes. There was no clear evidence that any active treatments were more acceptable to participants than any others. The relative effectiveness of intervention delivery modes must be taken into account in the context of the needs and preferences of individual young people, particularly as the differences between effect sizes were relatively small. Further research into the type and amount of therapist support that is most acceptable to young people and most cost-effective would be particularly useful.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
