Bryan Wu MD , Todd Atwood PhD, DABR , Arno J. Mundt MD , Jennifer Karunamuni MD , Paul Stark MD , Albert Hsiao MD, PhD , Frederick Han MD , Jonathan C. Hsu MD MAS , Kurt Hoffmayer MD PharmD , Farshad Raissi MD , Ulrika Birgersdotter-Green MD , Gregory Feld MD , David E. Krummen MD , Gordon Ho MD
{"title":"为室性心动过速的无创射频消融确定心脏收缩运动特征","authors":"Bryan Wu MD , Todd Atwood PhD, DABR , Arno J. Mundt MD , Jennifer Karunamuni MD , Paul Stark MD , Albert Hsiao MD, PhD , Frederick Han MD , Jonathan C. Hsu MD MAS , Kurt Hoffmayer MD PharmD , Farshad Raissi MD , Ulrika Birgersdotter-Green MD , Gregory Feld MD , David E. Krummen MD , Gordon Ho MD","doi":"10.1016/j.hroo.2023.12.006","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Respiratory motion management strategies are used to minimize the effects of breathing on the precision of stereotactic ablative radiotherapy for ventricular tachycardia, but the extent of cardiac contractile motion of the human heart has not been systematically explored.</p></div><div><h3>Objective</h3><p>We aim to assess the magnitude of cardiac contractile motion between different directions and locations in the heart.</p></div><div><h3>Methods</h3><p>Patients with intracardiac leads or valves who underwent 4-dimensional cardiac computed tomography (CT) prior to a catheter ablation procedure for atrial or ventricular arrhythmias at 2 medical centers were studied retrospectively. The displacement of transvenous right atrial appendage, right ventricular (RV) implantable cardioverter-defibrillator, coronary sinus lead tips, and prosthetic cardiac devices across the cardiac cycle were measured in orthogonal 3-dimensional views on a maximal-intensity projection CT reconstruction.</p></div><div><h3>Results</h3><p>A total of 31 preablation cardiac 4-dimensional cardiac CT scans were analyzed. The LV lead tip had significantly greater motion compared with the RV lead in the anterior-posterior direction (6.0 ± 2.2 mm vs 3.8 ± 1.7 mm; <em>P =</em> .01) and superior-inferior direction (4.4 ± 2.9 mm vs 3.5 ± 2.0 mm; <em>P =</em> .049). The prosthetic aortic valves had the least movement of all fiducials, specifically compared with the RV lead tip in the left-right direction (3.2 ± 1.2 mm vs 6.1 ± 3.8 mm, <em>P =</em> .04) and the LV lead tip in the anterior-posterior direction (3.8 ± 1.7 mm vs 6.0 ± 2.2 mm, <em>P =</em> .03).</p></div><div><h3>Conclusion</h3><p>The degree of cardiac contractile motion varies significantly (1 mm to 15.2 mm) across different locations in the heart. The effect of contractile motion on the precision of radiotherapy should be assessed on a patient-specific basis.</p></div>","PeriodicalId":29772,"journal":{"name":"Heart Rhythm O2","volume":"5 2","pages":"Pages 131-136"},"PeriodicalIF":2.8000,"publicationDate":"2024-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S2666501823003367/pdfft?md5=2949eb2bc7066c6e2844bf7355d4008d&pid=1-s2.0-S2666501823003367-main.pdf","citationCount":"0","resultStr":"{\"title\":\"Characterizing cardiac contractile motion for noninvasive radioablation of ventricular tachycardia\",\"authors\":\"Bryan Wu MD , Todd Atwood PhD, DABR , Arno J. Mundt MD , Jennifer Karunamuni MD , Paul Stark MD , Albert Hsiao MD, PhD , Frederick Han MD , Jonathan C. Hsu MD MAS , Kurt Hoffmayer MD PharmD , Farshad Raissi MD , Ulrika Birgersdotter-Green MD , Gregory Feld MD , David E. Krummen MD , Gordon Ho MD\",\"doi\":\"10.1016/j.hroo.2023.12.006\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>Respiratory motion management strategies are used to minimize the effects of breathing on the precision of stereotactic ablative radiotherapy for ventricular tachycardia, but the extent of cardiac contractile motion of the human heart has not been systematically explored.</p></div><div><h3>Objective</h3><p>We aim to assess the magnitude of cardiac contractile motion between different directions and locations in the heart.</p></div><div><h3>Methods</h3><p>Patients with intracardiac leads or valves who underwent 4-dimensional cardiac computed tomography (CT) prior to a catheter ablation procedure for atrial or ventricular arrhythmias at 2 medical centers were studied retrospectively. The displacement of transvenous right atrial appendage, right ventricular (RV) implantable cardioverter-defibrillator, coronary sinus lead tips, and prosthetic cardiac devices across the cardiac cycle were measured in orthogonal 3-dimensional views on a maximal-intensity projection CT reconstruction.</p></div><div><h3>Results</h3><p>A total of 31 preablation cardiac 4-dimensional cardiac CT scans were analyzed. The LV lead tip had significantly greater motion compared with the RV lead in the anterior-posterior direction (6.0 ± 2.2 mm vs 3.8 ± 1.7 mm; <em>P =</em> .01) and superior-inferior direction (4.4 ± 2.9 mm vs 3.5 ± 2.0 mm; <em>P =</em> .049). The prosthetic aortic valves had the least movement of all fiducials, specifically compared with the RV lead tip in the left-right direction (3.2 ± 1.2 mm vs 6.1 ± 3.8 mm, <em>P =</em> .04) and the LV lead tip in the anterior-posterior direction (3.8 ± 1.7 mm vs 6.0 ± 2.2 mm, <em>P =</em> .03).</p></div><div><h3>Conclusion</h3><p>The degree of cardiac contractile motion varies significantly (1 mm to 15.2 mm) across different locations in the heart. The effect of contractile motion on the precision of radiotherapy should be assessed on a patient-specific basis.</p></div>\",\"PeriodicalId\":29772,\"journal\":{\"name\":\"Heart Rhythm O2\",\"volume\":\"5 2\",\"pages\":\"Pages 131-136\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2024-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.sciencedirect.com/science/article/pii/S2666501823003367/pdfft?md5=2949eb2bc7066c6e2844bf7355d4008d&pid=1-s2.0-S2666501823003367-main.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Heart Rhythm O2\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2666501823003367\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/12/23 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Heart Rhythm O2","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2666501823003367","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/12/23 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景呼吸运动管理策略用于最大限度地减少呼吸对室性心动过速立体定向消融放疗精确性的影响,但对人体心脏收缩运动的程度尚未进行系统的探讨。方法回顾性研究了在两家医疗中心接受导管消融术治疗房性或室性心律失常的心内导联或瓣膜患者,这些患者在接受导管消融术前都接受了四维心脏计算机断层扫描(CT)。在最大强度投影 CT 重建的正交三维视图中测量了经静脉右房阑尾、右心室 (RV) 植入式心律转复除颤器、冠状窦导联尖端和人工心脏装置在整个心动周期中的位移。在前后方向(6.0 ± 2.2 mm vs 3.8 ± 1.7 mm;P = .01)和上下方向(4.4 ± 2.9 mm vs 3.5 ± 2.0 mm;P = .049),左心室导联尖端的运动明显大于右心室导联。在所有靶标中,人工主动脉瓣的运动最小,特别是与左心室导联尖在左右方向(3.2 ± 1.2 mm vs 6.1 ± 3.8 mm,P = .04)和左心室导联尖在前后方向(3.8 ± 1.7 mm vs 6.0 ± 2.2 mm,P = .03)相比。应根据患者的具体情况评估收缩运动对放疗精确度的影响。
Characterizing cardiac contractile motion for noninvasive radioablation of ventricular tachycardia
Background
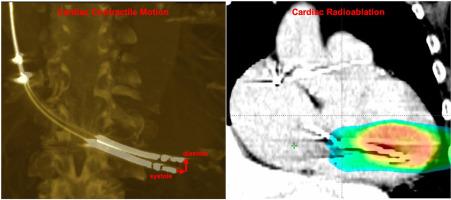
Respiratory motion management strategies are used to minimize the effects of breathing on the precision of stereotactic ablative radiotherapy for ventricular tachycardia, but the extent of cardiac contractile motion of the human heart has not been systematically explored.
Objective
We aim to assess the magnitude of cardiac contractile motion between different directions and locations in the heart.
Methods
Patients with intracardiac leads or valves who underwent 4-dimensional cardiac computed tomography (CT) prior to a catheter ablation procedure for atrial or ventricular arrhythmias at 2 medical centers were studied retrospectively. The displacement of transvenous right atrial appendage, right ventricular (RV) implantable cardioverter-defibrillator, coronary sinus lead tips, and prosthetic cardiac devices across the cardiac cycle were measured in orthogonal 3-dimensional views on a maximal-intensity projection CT reconstruction.
Results
A total of 31 preablation cardiac 4-dimensional cardiac CT scans were analyzed. The LV lead tip had significantly greater motion compared with the RV lead in the anterior-posterior direction (6.0 ± 2.2 mm vs 3.8 ± 1.7 mm; P = .01) and superior-inferior direction (4.4 ± 2.9 mm vs 3.5 ± 2.0 mm; P = .049). The prosthetic aortic valves had the least movement of all fiducials, specifically compared with the RV lead tip in the left-right direction (3.2 ± 1.2 mm vs 6.1 ± 3.8 mm, P = .04) and the LV lead tip in the anterior-posterior direction (3.8 ± 1.7 mm vs 6.0 ± 2.2 mm, P = .03).
Conclusion
The degree of cardiac contractile motion varies significantly (1 mm to 15.2 mm) across different locations in the heart. The effect of contractile motion on the precision of radiotherapy should be assessed on a patient-specific basis.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
