{"title":"印度对转移性激素敏感性前列腺癌加强治疗的系统疗法成本效益分析。","authors":"Nidhi Gupta, Dharna Gupta, Kiran Gopal Vaska, Shankar Prinja","doi":"10.1007/s40258-023-00866-w","DOIUrl":null,"url":null,"abstract":"<div><h3>Background and Objective</h3><p>Androgen-deprivation therapy is the mainstay of treatment for patients with newly diagnosed metastatic hormone-sensitive prostate cancer (mHSPC). However, the intensification of treatment with either docetaxel or novel anti-androgens (abiraterone-acetate plus prednisone [AAP], enzalutamide, and apalutamide) is being recommended based on the improved clinical outcomes and quality of life among patients. This study aimed to determine the most cost-effective drug for treatment intensification for patients with mHSPC in India.</p><h3>Methods</h3><p>A Markov model was developed with four health states: progression-free survival, progressive disease, best supportive care, and death. Lifetime costs and consequences were estimated for four treatment sequences: AAP-first, enzalutamide-first, apalutamide-first, and docetaxel-first. Incremental cost per quality-adjusted life-year (QALY) gained with a given treatment option was compared against the next best alternative and assessed for cost effectiveness using a willingness to pay threshold of 1 × per capita gross domestic product in India.</p><h3>Results</h3><p>We estimated that the total lifetime cost per patient was ₹1,367,454 (US$17,487), ₹2,168,885 (US$27,735), ₹7,678,501 (US$98,190), and ₹1,358,746 (US$17,375) in the AAP-first, enzalutamide-first, apalutamide-first, and docetaxel-first treatment sequence, respectively. The mean quality-adjusted life-years lived per patient were 4.78, 5.03, 3.22, and 2.61, respectively. The AAP-first sequence incurs an incremental cost of ₹4014 (US$51) per quality-adjusted life-year gained as compared with the docetaxel-first sequence, with a 87% probability of being cost effective at the willingness-to-pay threshold of 1 × per-capita gross domestic product of India. The use of AAP-first also incurs an incremental net monetary benefit of ₹396,491 (US$5070) as compared with the docetaxel-first treatment sequence. Nearly a 48% reduction in the price of enzalutamide is required to make it a cost-effective treatment sequence as compared with AAP-first in India.</p><h3>Conclusions</h3><p>We concur with the inclusion of standard-dose AAP in India’s publicly financed health insurance scheme for the intensification of treatment in mHSPC as it is the only cost-effective sequence among the various novel anti-androgens when compared with the docetaxel-first treatment sequence. Furthermore, a systematic reduction in the price of enzalutamide would further help to improve clinical outcomes among patients with mHSPC.</p></div>","PeriodicalId":8065,"journal":{"name":"Applied Health Economics and Health Policy","volume":"22 3","pages":"415 - 426"},"PeriodicalIF":3.3000,"publicationDate":"2024-01-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Cost-Effectiveness Analysis of Systemic Therapy for Intensification of Treatment in Metastatic Hormone-Sensitive Prostate Cancer in India\",\"authors\":\"Nidhi Gupta, Dharna Gupta, Kiran Gopal Vaska, Shankar Prinja\",\"doi\":\"10.1007/s40258-023-00866-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background and Objective</h3><p>Androgen-deprivation therapy is the mainstay of treatment for patients with newly diagnosed metastatic hormone-sensitive prostate cancer (mHSPC). However, the intensification of treatment with either docetaxel or novel anti-androgens (abiraterone-acetate plus prednisone [AAP], enzalutamide, and apalutamide) is being recommended based on the improved clinical outcomes and quality of life among patients. This study aimed to determine the most cost-effective drug for treatment intensification for patients with mHSPC in India.</p><h3>Methods</h3><p>A Markov model was developed with four health states: progression-free survival, progressive disease, best supportive care, and death. Lifetime costs and consequences were estimated for four treatment sequences: AAP-first, enzalutamide-first, apalutamide-first, and docetaxel-first. Incremental cost per quality-adjusted life-year (QALY) gained with a given treatment option was compared against the next best alternative and assessed for cost effectiveness using a willingness to pay threshold of 1 × per capita gross domestic product in India.</p><h3>Results</h3><p>We estimated that the total lifetime cost per patient was ₹1,367,454 (US$17,487), ₹2,168,885 (US$27,735), ₹7,678,501 (US$98,190), and ₹1,358,746 (US$17,375) in the AAP-first, enzalutamide-first, apalutamide-first, and docetaxel-first treatment sequence, respectively. The mean quality-adjusted life-years lived per patient were 4.78, 5.03, 3.22, and 2.61, respectively. The AAP-first sequence incurs an incremental cost of ₹4014 (US$51) per quality-adjusted life-year gained as compared with the docetaxel-first sequence, with a 87% probability of being cost effective at the willingness-to-pay threshold of 1 × per-capita gross domestic product of India. The use of AAP-first also incurs an incremental net monetary benefit of ₹396,491 (US$5070) as compared with the docetaxel-first treatment sequence. Nearly a 48% reduction in the price of enzalutamide is required to make it a cost-effective treatment sequence as compared with AAP-first in India.</p><h3>Conclusions</h3><p>We concur with the inclusion of standard-dose AAP in India’s publicly financed health insurance scheme for the intensification of treatment in mHSPC as it is the only cost-effective sequence among the various novel anti-androgens when compared with the docetaxel-first treatment sequence. Furthermore, a systematic reduction in the price of enzalutamide would further help to improve clinical outcomes among patients with mHSPC.</p></div>\",\"PeriodicalId\":8065,\"journal\":{\"name\":\"Applied Health Economics and Health Policy\",\"volume\":\"22 3\",\"pages\":\"415 - 426\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2024-01-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Applied Health Economics and Health Policy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://link.springer.com/article/10.1007/s40258-023-00866-w\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ECONOMICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Applied Health Economics and Health Policy","FirstCategoryId":"3","ListUrlMain":"https://link.springer.com/article/10.1007/s40258-023-00866-w","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ECONOMICS","Score":null,"Total":0}
Cost-Effectiveness Analysis of Systemic Therapy for Intensification of Treatment in Metastatic Hormone-Sensitive Prostate Cancer in India
Background and Objective
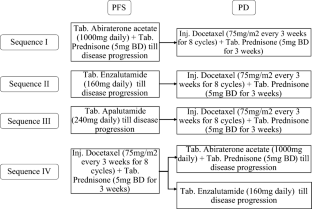
Androgen-deprivation therapy is the mainstay of treatment for patients with newly diagnosed metastatic hormone-sensitive prostate cancer (mHSPC). However, the intensification of treatment with either docetaxel or novel anti-androgens (abiraterone-acetate plus prednisone [AAP], enzalutamide, and apalutamide) is being recommended based on the improved clinical outcomes and quality of life among patients. This study aimed to determine the most cost-effective drug for treatment intensification for patients with mHSPC in India.
Methods
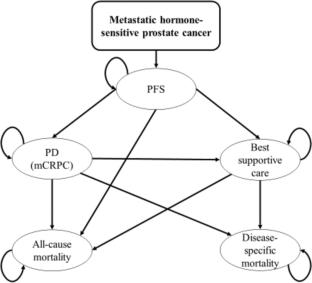
A Markov model was developed with four health states: progression-free survival, progressive disease, best supportive care, and death. Lifetime costs and consequences were estimated for four treatment sequences: AAP-first, enzalutamide-first, apalutamide-first, and docetaxel-first. Incremental cost per quality-adjusted life-year (QALY) gained with a given treatment option was compared against the next best alternative and assessed for cost effectiveness using a willingness to pay threshold of 1 × per capita gross domestic product in India.
Results
We estimated that the total lifetime cost per patient was ₹1,367,454 (US$17,487), ₹2,168,885 (US$27,735), ₹7,678,501 (US$98,190), and ₹1,358,746 (US$17,375) in the AAP-first, enzalutamide-first, apalutamide-first, and docetaxel-first treatment sequence, respectively. The mean quality-adjusted life-years lived per patient were 4.78, 5.03, 3.22, and 2.61, respectively. The AAP-first sequence incurs an incremental cost of ₹4014 (US$51) per quality-adjusted life-year gained as compared with the docetaxel-first sequence, with a 87% probability of being cost effective at the willingness-to-pay threshold of 1 × per-capita gross domestic product of India. The use of AAP-first also incurs an incremental net monetary benefit of ₹396,491 (US$5070) as compared with the docetaxel-first treatment sequence. Nearly a 48% reduction in the price of enzalutamide is required to make it a cost-effective treatment sequence as compared with AAP-first in India.
Conclusions
We concur with the inclusion of standard-dose AAP in India’s publicly financed health insurance scheme for the intensification of treatment in mHSPC as it is the only cost-effective sequence among the various novel anti-androgens when compared with the docetaxel-first treatment sequence. Furthermore, a systematic reduction in the price of enzalutamide would further help to improve clinical outcomes among patients with mHSPC.
期刊介绍:
Applied Health Economics and Health Policy provides timely publication of cutting-edge research and expert opinion from this increasingly important field, making it a vital resource for payers, providers and researchers alike. The journal includes high quality economic research and reviews of all aspects of healthcare from various perspectives and countries, designed to communicate the latest applied information in health economics and health policy.
While emphasis is placed on information with practical applications, a strong basis of underlying scientific rigor is maintained.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
