Ellen T Chang, Christina A Clarke, Graham A Colditz, Allison W Kurian, Earl Hubbell
{"title":"通过估算癌症和非癌症死亡的特定阶段比例来避免提前期偏差。","authors":"Ellen T Chang, Christina A Clarke, Graham A Colditz, Allison W Kurian, Earl Hubbell","doi":"10.1007/s10552-023-01842-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Understanding how stage at cancer diagnosis influences cause of death, an endpoint that is not susceptible to lead-time bias, can inform population-level outcomes of cancer screening.</p><p><strong>Methods: </strong>Using data from 17 US Surveillance, Epidemiology, and End Results registries for 1,154,515 persons aged 50-84 years at cancer diagnosis in 2006-2010, we evaluated proportional causes of death by cancer type and uniformly classified stage, following or extrapolating all patients until death through 2020.</p><p><strong>Results: </strong>Most cancer patients diagnosed at stages I-II did not go on to die from their index cancer, whereas most patients diagnosed at stage IV did. For patients diagnosed with any cancer at stages I-II, an estimated 26% of deaths were due to the index cancer, 63% due to non-cancer causes, and 12% due to a subsequent primary (non-index) cancer. In contrast, for patients diagnosed with any stage IV cancer, 85% of deaths were attributed to the index cancer, with 13% non-cancer and 2% non-index-cancer deaths. Index cancer mortality from stages I-II cancer was proportionally lowest for thyroid, melanoma, uterus, prostate, and breast, and highest for pancreas, liver, esophagus, lung, and stomach.</p><p><strong>Conclusion: </strong>Across all cancer types, the percentage of patients who went on to die from their cancer was over three times greater when the cancer was diagnosed at stage IV than stages I-II. As mortality patterns are not influenced by lead-time bias, these data suggest that earlier detection is likely to improve outcomes across cancer types, including those currently unscreened.</p>","PeriodicalId":9432,"journal":{"name":"Cancer Causes & Control","volume":" ","pages":"849-864"},"PeriodicalIF":2.1000,"publicationDate":"2024-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11045653/pdf/","citationCount":"0","resultStr":"{\"title\":\"Avoiding lead-time bias by estimating stage-specific proportions of cancer and non-cancer deaths.\",\"authors\":\"Ellen T Chang, Christina A Clarke, Graham A Colditz, Allison W Kurian, Earl Hubbell\",\"doi\":\"10.1007/s10552-023-01842-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>Understanding how stage at cancer diagnosis influences cause of death, an endpoint that is not susceptible to lead-time bias, can inform population-level outcomes of cancer screening.</p><p><strong>Methods: </strong>Using data from 17 US Surveillance, Epidemiology, and End Results registries for 1,154,515 persons aged 50-84 years at cancer diagnosis in 2006-2010, we evaluated proportional causes of death by cancer type and uniformly classified stage, following or extrapolating all patients until death through 2020.</p><p><strong>Results: </strong>Most cancer patients diagnosed at stages I-II did not go on to die from their index cancer, whereas most patients diagnosed at stage IV did. For patients diagnosed with any cancer at stages I-II, an estimated 26% of deaths were due to the index cancer, 63% due to non-cancer causes, and 12% due to a subsequent primary (non-index) cancer. In contrast, for patients diagnosed with any stage IV cancer, 85% of deaths were attributed to the index cancer, with 13% non-cancer and 2% non-index-cancer deaths. Index cancer mortality from stages I-II cancer was proportionally lowest for thyroid, melanoma, uterus, prostate, and breast, and highest for pancreas, liver, esophagus, lung, and stomach.</p><p><strong>Conclusion: </strong>Across all cancer types, the percentage of patients who went on to die from their cancer was over three times greater when the cancer was diagnosed at stage IV than stages I-II. As mortality patterns are not influenced by lead-time bias, these data suggest that earlier detection is likely to improve outcomes across cancer types, including those currently unscreened.</p>\",\"PeriodicalId\":9432,\"journal\":{\"name\":\"Cancer Causes & Control\",\"volume\":\" \",\"pages\":\"849-864\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2024-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11045653/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cancer Causes & Control\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10552-023-01842-4\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/18 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Causes & Control","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10552-023-01842-4","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/18 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
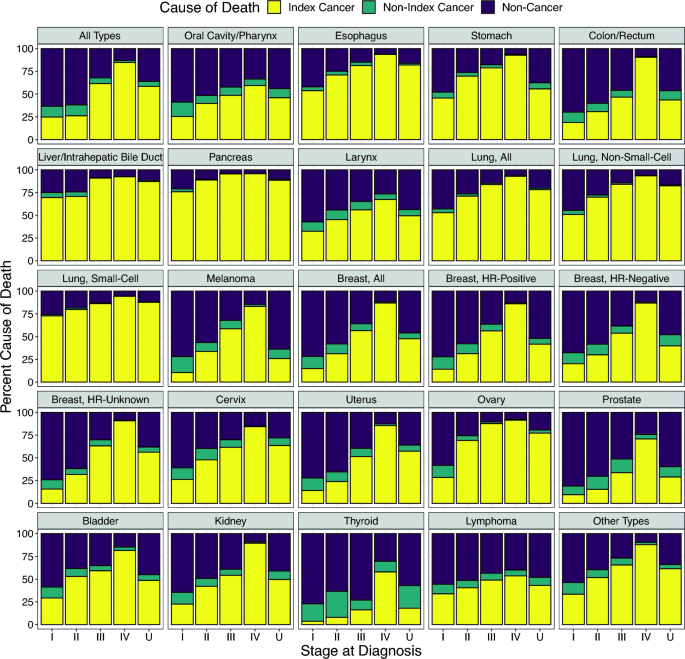
Avoiding lead-time bias by estimating stage-specific proportions of cancer and non-cancer deaths.
Purpose: Understanding how stage at cancer diagnosis influences cause of death, an endpoint that is not susceptible to lead-time bias, can inform population-level outcomes of cancer screening.
Methods: Using data from 17 US Surveillance, Epidemiology, and End Results registries for 1,154,515 persons aged 50-84 years at cancer diagnosis in 2006-2010, we evaluated proportional causes of death by cancer type and uniformly classified stage, following or extrapolating all patients until death through 2020.
Results: Most cancer patients diagnosed at stages I-II did not go on to die from their index cancer, whereas most patients diagnosed at stage IV did. For patients diagnosed with any cancer at stages I-II, an estimated 26% of deaths were due to the index cancer, 63% due to non-cancer causes, and 12% due to a subsequent primary (non-index) cancer. In contrast, for patients diagnosed with any stage IV cancer, 85% of deaths were attributed to the index cancer, with 13% non-cancer and 2% non-index-cancer deaths. Index cancer mortality from stages I-II cancer was proportionally lowest for thyroid, melanoma, uterus, prostate, and breast, and highest for pancreas, liver, esophagus, lung, and stomach.
Conclusion: Across all cancer types, the percentage of patients who went on to die from their cancer was over three times greater when the cancer was diagnosed at stage IV than stages I-II. As mortality patterns are not influenced by lead-time bias, these data suggest that earlier detection is likely to improve outcomes across cancer types, including those currently unscreened.
期刊介绍:
Cancer Causes & Control is an international refereed journal that both reports and stimulates new avenues of investigation into the causes, control, and subsequent prevention of cancer. By drawing together related information published currently in a diverse range of biological and medical journals, it has a multidisciplinary and multinational approach.
The scope of the journal includes: variation in cancer distribution within and between populations; factors associated with cancer risk; preventive and therapeutic interventions on a population scale; economic, demographic, and health-policy implications of cancer; and related methodological issues.
The emphasis is on speed of publication. The journal will normally publish within 30 to 60 days of acceptance of manuscripts.
Cancer Causes & Control publishes Original Articles, Reviews, Commentaries, Opinions, Short Communications and Letters to the Editor which will have direct relevance to researchers and practitioners working in epidemiology, medical statistics, cancer biology, health education, medical economics and related fields. The journal also contains significant information for government agencies concerned with cancer research, control and policy.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
