Johanna Eichinger, Andrea Büchler, Louisa Arnold, Michael Rost
{"title":"妇女和助产士关于分娩中是否允许胁迫的道德推理:一项描述性伦理研究。","authors":"Johanna Eichinger, Andrea Büchler, Louisa Arnold, Michael Rost","doi":"10.1007/s10728-024-00480-4","DOIUrl":null,"url":null,"abstract":"<p><p>Evidence shows that during birth women frequently experience unconsented care, coercion, and a loss of autonomy. For many countries, this contradicts both the law and medical ethics guidelines, which emphasize that competent and fully informed women's autonomy must always be respected. To better understand this discordance, we empirically describe perinatal maternity care providers' and women's moral deliberation surrounding coercive measures during birth. Data were obtained from 1-on-1 interviews with providers (N = 15) and women (N = 14), and a survey of women (N = 118). Analyses focused on an in-depth exploration of responses to a question on the permissibility of coercion in birth whose wording was borrowed from a Swiss medical-ethical guideline. Reasons for and against a principle permissibility of coercive measures in birth were grouped into clusters of reasons to build a coherent explanatory framework. Factors considered morally relevant when deliberating on coercion included women's decisional capacity, beneficence/non-maleficence, authority through knowledge on the part of providers, flaws of the medical system, or the imperative to protect the most vulnerable. Also, we identified various misconceptions, such as the conviction that a pathological birth can justify coercion or that fetal rights can justifiably infringe on women's autonomy. Information and education on the issue of coercion in birth are urgently needed to enable women to fully exercise their reproductive autonomy, to prevent long-term adverse health outcomes of women and children, and to reconcile the medical vigilance which has lead to a reduction of perinatal morbidity and mortality with women's enfranchisement in their own care.</p>","PeriodicalId":46740,"journal":{"name":"Health Care Analysis","volume":" ","pages":"184-204"},"PeriodicalIF":1.6000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11390788/pdf/","citationCount":"0","resultStr":"{\"title\":\"Women's and Provider's Moral Reasoning About the Permissibility of Coercion in Birth: A Descriptive Ethics Study.\",\"authors\":\"Johanna Eichinger, Andrea Büchler, Louisa Arnold, Michael Rost\",\"doi\":\"10.1007/s10728-024-00480-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Evidence shows that during birth women frequently experience unconsented care, coercion, and a loss of autonomy. For many countries, this contradicts both the law and medical ethics guidelines, which emphasize that competent and fully informed women's autonomy must always be respected. To better understand this discordance, we empirically describe perinatal maternity care providers' and women's moral deliberation surrounding coercive measures during birth. Data were obtained from 1-on-1 interviews with providers (N = 15) and women (N = 14), and a survey of women (N = 118). Analyses focused on an in-depth exploration of responses to a question on the permissibility of coercion in birth whose wording was borrowed from a Swiss medical-ethical guideline. Reasons for and against a principle permissibility of coercive measures in birth were grouped into clusters of reasons to build a coherent explanatory framework. Factors considered morally relevant when deliberating on coercion included women's decisional capacity, beneficence/non-maleficence, authority through knowledge on the part of providers, flaws of the medical system, or the imperative to protect the most vulnerable. Also, we identified various misconceptions, such as the conviction that a pathological birth can justify coercion or that fetal rights can justifiably infringe on women's autonomy. Information and education on the issue of coercion in birth are urgently needed to enable women to fully exercise their reproductive autonomy, to prevent long-term adverse health outcomes of women and children, and to reconcile the medical vigilance which has lead to a reduction of perinatal morbidity and mortality with women's enfranchisement in their own care.</p>\",\"PeriodicalId\":46740,\"journal\":{\"name\":\"Health Care Analysis\",\"volume\":\" \",\"pages\":\"184-204\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2024-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11390788/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Health Care Analysis\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s10728-024-00480-4\",\"RegionNum\":3,\"RegionCategory\":\"哲学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/23 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"ETHICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health Care Analysis","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10728-024-00480-4","RegionNum":3,"RegionCategory":"哲学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/23 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ETHICS","Score":null,"Total":0}
Women's and Provider's Moral Reasoning About the Permissibility of Coercion in Birth: A Descriptive Ethics Study.
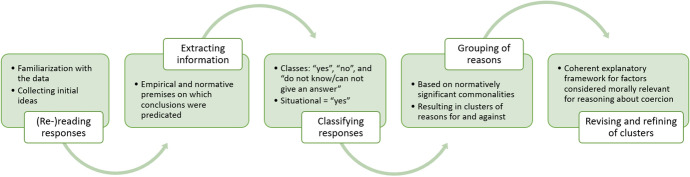
Evidence shows that during birth women frequently experience unconsented care, coercion, and a loss of autonomy. For many countries, this contradicts both the law and medical ethics guidelines, which emphasize that competent and fully informed women's autonomy must always be respected. To better understand this discordance, we empirically describe perinatal maternity care providers' and women's moral deliberation surrounding coercive measures during birth. Data were obtained from 1-on-1 interviews with providers (N = 15) and women (N = 14), and a survey of women (N = 118). Analyses focused on an in-depth exploration of responses to a question on the permissibility of coercion in birth whose wording was borrowed from a Swiss medical-ethical guideline. Reasons for and against a principle permissibility of coercive measures in birth were grouped into clusters of reasons to build a coherent explanatory framework. Factors considered morally relevant when deliberating on coercion included women's decisional capacity, beneficence/non-maleficence, authority through knowledge on the part of providers, flaws of the medical system, or the imperative to protect the most vulnerable. Also, we identified various misconceptions, such as the conviction that a pathological birth can justify coercion or that fetal rights can justifiably infringe on women's autonomy. Information and education on the issue of coercion in birth are urgently needed to enable women to fully exercise their reproductive autonomy, to prevent long-term adverse health outcomes of women and children, and to reconcile the medical vigilance which has lead to a reduction of perinatal morbidity and mortality with women's enfranchisement in their own care.
期刊介绍:
Health Care Analysis is a journal that promotes dialogue and debate about conceptual and normative issues related to health and health care, including health systems, healthcare provision, health law, public policy and health, professional health practice, health services organization and decision-making, and health-related education at all levels of clinical medicine, public health and global health. Health Care Analysis seeks to support the conversation between philosophy and policy, in particular illustrating the importance of conceptual and normative analysis to health policy, practice and research. As such, papers accepted for publication are likely to analyse philosophical questions related to health, health care or health policy that focus on one or more of the following: aims or ends, theories, frameworks, concepts, principles, values or ideology. All styles of theoretical analysis are welcome providing that they illuminate conceptual or normative issues and encourage debate between those interested in health, philosophy and policy. Papers must be rigorous, but should strive for accessibility – with care being taken to ensure that their arguments and implications are plain to a broad academic and international audience. In addition to purely theoretical papers, papers grounded in empirical research or case-studies are very welcome so long as they explore the conceptual or normative implications of such work. Authors are encouraged, where possible, to have regard to the social contexts of the issues they are discussing, and all authors should ensure that they indicate the ‘real world’ implications of their work. Health Care Analysis publishes contributions from philosophers, lawyers, social scientists, healthcare educators, healthcare professionals and administrators, and other health-related academics and policy analysts.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
