{"title":"炎症性肠病专科医生与保险授权拒绝之间的不一致--特定炎症性肠病治疗方案调查》(Inflammatory Bowel Disease Specialists and Insurance Authorization Denials-A Survey of Specific Inflammatory Bowel Disease Treatment Scenarios)。","authors":"Anastasia Naritsin, Neev Mehta, Randall Pellish","doi":"10.1093/crocol/otad082","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Prior authorizations are generally required by insurers for gastroenterologists to prescribe biologics and small-molecule drugs to treat inflammatory bowel disease (IBD). Authorization denials occur in a wide variety of clinical scenarios, including denials of standard and nonstandard medication dosing.</p><p><strong>Methods: </strong>We performed a national cross-sectional survey on a broad variety of specific clinical scenarios to assess experience and opinions on whether or not insurance authorization denials are in accordance with clinical expertise.</p><p><strong>Results: </strong>Eighty-four gastroenterologists completed the survey. Denial experience was common for infliximab dose modifications, vedolizumab dose modifications, ustekinumab first-time therapy, and maintenance dosing. The bulk of disagreement with authorization denials involved scenarios of dose escalation and re-induction guided by both loss of clinical response and/or therapeutic drug monitoring, denial of re-authorizations of stable dosing, and use of non-anti-TNFs in specific patient populations including the elderly and patients with multiple comorbidities. Respondents unanimously agreed that insurance companies do not play an adequate role in helping patients obtain PA. Furthermore, most of the respondents agree that to decrease the burden of the PA process, peer-peer processes should be between other IBD-trained providers who understand these complex treatment strategies.</p><p><strong>Conclusions: </strong>Our cross-sectional survey highlights the degree of discordance in clinical decision-making between insurers and gastroenterologists. Further engagement between gastroenterologists and insurers is needed to foster common understanding on these discordant authorization denials in these real-world clinical IBD scenarios.</p>","PeriodicalId":10847,"journal":{"name":"Crohn's & Colitis 360","volume":"6 1","pages":"otad082"},"PeriodicalIF":1.8000,"publicationDate":"2023-12-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10805526/pdf/","citationCount":"0","resultStr":"{\"title\":\"Discordance Between Inflammatory Bowel Disease Specialists and Insurance Authorization Denials-A Survey of Specific Inflammatory Bowel Disease Treatment Scenarios.\",\"authors\":\"Anastasia Naritsin, Neev Mehta, Randall Pellish\",\"doi\":\"10.1093/crocol/otad082\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Prior authorizations are generally required by insurers for gastroenterologists to prescribe biologics and small-molecule drugs to treat inflammatory bowel disease (IBD). Authorization denials occur in a wide variety of clinical scenarios, including denials of standard and nonstandard medication dosing.</p><p><strong>Methods: </strong>We performed a national cross-sectional survey on a broad variety of specific clinical scenarios to assess experience and opinions on whether or not insurance authorization denials are in accordance with clinical expertise.</p><p><strong>Results: </strong>Eighty-four gastroenterologists completed the survey. Denial experience was common for infliximab dose modifications, vedolizumab dose modifications, ustekinumab first-time therapy, and maintenance dosing. The bulk of disagreement with authorization denials involved scenarios of dose escalation and re-induction guided by both loss of clinical response and/or therapeutic drug monitoring, denial of re-authorizations of stable dosing, and use of non-anti-TNFs in specific patient populations including the elderly and patients with multiple comorbidities. Respondents unanimously agreed that insurance companies do not play an adequate role in helping patients obtain PA. Furthermore, most of the respondents agree that to decrease the burden of the PA process, peer-peer processes should be between other IBD-trained providers who understand these complex treatment strategies.</p><p><strong>Conclusions: </strong>Our cross-sectional survey highlights the degree of discordance in clinical decision-making between insurers and gastroenterologists. Further engagement between gastroenterologists and insurers is needed to foster common understanding on these discordant authorization denials in these real-world clinical IBD scenarios.</p>\",\"PeriodicalId\":10847,\"journal\":{\"name\":\"Crohn's & Colitis 360\",\"volume\":\"6 1\",\"pages\":\"otad082\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2023-12-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10805526/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Crohn's & Colitis 360\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/crocol/otad082\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Crohn's & Colitis 360","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/crocol/otad082","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
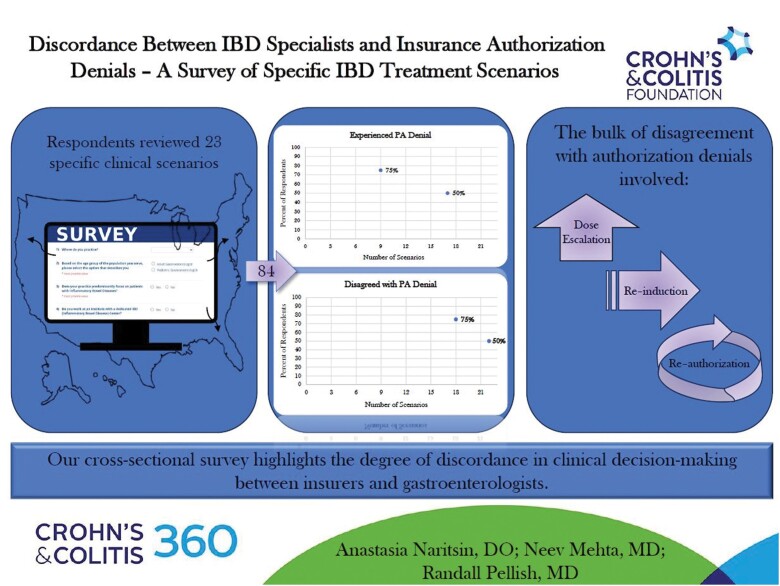
背景:保险公司通常要求肠胃病专家在处方治疗炎症性肠病(IBD)的生物制剂和小分子药物时必须获得预先授权。拒绝授权的临床情况多种多样,包括拒绝标准和非标准药物剂量:我们就各种特定的临床情况进行了一次全国性横断面调查,以评估保险拒保是否符合临床专业知识的经验和观点:84名消化科医生完成了调查。在英夫利西单抗剂量调整、维妥珠单抗剂量调整、乌斯特库单抗首次治疗和维持剂量方面,拒绝授权的情况很常见。对拒绝授权的异议主要涉及临床反应消失和/或治疗药物监测指导下的剂量升级和再减量、拒绝重新授权稳定剂量,以及在特定患者群体(包括老年人和有多种并发症的患者)中使用非抗-TNFs。受访者一致认为,保险公司在帮助患者获得 PA 方面没有发挥足够的作用。此外,大多数受访者都认为,为了减轻 PA 程序的负担,应在其他受过 IBD 培训、了解这些复杂治疗策略的医疗服务提供者之间开展同行间的程序:我们的横向调查凸显了保险公司与消化内科医生在临床决策方面的不一致程度。胃肠病学家和保险公司之间需要进一步接触,以便在这些真实的 IBD 临床场景中就这些不一致的授权拒绝达成共识。
Discordance Between Inflammatory Bowel Disease Specialists and Insurance Authorization Denials-A Survey of Specific Inflammatory Bowel Disease Treatment Scenarios.
Background: Prior authorizations are generally required by insurers for gastroenterologists to prescribe biologics and small-molecule drugs to treat inflammatory bowel disease (IBD). Authorization denials occur in a wide variety of clinical scenarios, including denials of standard and nonstandard medication dosing.
Methods: We performed a national cross-sectional survey on a broad variety of specific clinical scenarios to assess experience and opinions on whether or not insurance authorization denials are in accordance with clinical expertise.
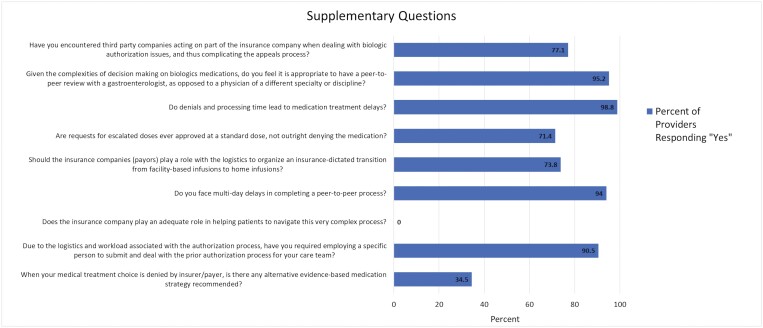
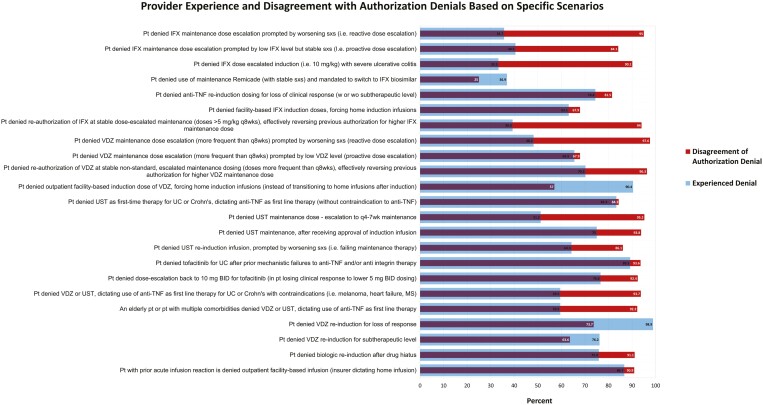
Results: Eighty-four gastroenterologists completed the survey. Denial experience was common for infliximab dose modifications, vedolizumab dose modifications, ustekinumab first-time therapy, and maintenance dosing. The bulk of disagreement with authorization denials involved scenarios of dose escalation and re-induction guided by both loss of clinical response and/or therapeutic drug monitoring, denial of re-authorizations of stable dosing, and use of non-anti-TNFs in specific patient populations including the elderly and patients with multiple comorbidities. Respondents unanimously agreed that insurance companies do not play an adequate role in helping patients obtain PA. Furthermore, most of the respondents agree that to decrease the burden of the PA process, peer-peer processes should be between other IBD-trained providers who understand these complex treatment strategies.
Conclusions: Our cross-sectional survey highlights the degree of discordance in clinical decision-making between insurers and gastroenterologists. Further engagement between gastroenterologists and insurers is needed to foster common understanding on these discordant authorization denials in these real-world clinical IBD scenarios.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
