Patricia E Penovich, Vikram R Rao, Lucretia Long, Enrique Carrazana, Adrian L Rabinowicz
{"title":"苯二氮卓类药物治疗癫痫发作群。","authors":"Patricia E Penovich, Vikram R Rao, Lucretia Long, Enrique Carrazana, Adrian L Rabinowicz","doi":"10.1007/s40263-023-01060-1","DOIUrl":null,"url":null,"abstract":"<p><p>Patients with epilepsy may experience seizure clusters, which are described by the US Food and Drug Administration (FDA) as intermittent, stereotypic episodes of frequent seizure activity that are distinct from a patient's usual seizure pattern. Untreated seizure clusters may increase the risk for status epilepticus, as well as decrease quality of life and increase burden on patients and care partners. Benzodiazepine therapies are the mainstay for acute treatment of seizure clusters and are often administered by nonmedical care partners outside a healthcare facility. Three rescue therapies are currently FDA-approved for this indication, with diazepam rectal gel being the first in 1997, for patients aged ≥ 2 years. Limitations of rectal administration (e.g., positioning and disrobing the patient, which may affect ease of use and social acceptability; interpatient variation in bioavailability) led to the investigation of the potential for nasal administration as an alternative. Midazolam nasal spray (MDS) was approved by the FDA in 2019 for patients aged ≥ 12 years and diazepam nasal spray (DNS) in 2020 for patients aged ≥ 6 years; these two intranasal therapies have differences in their formulations [e.g., organic solvents (MDS) vs. Intravail and vitamin E for absorption and solubility (DNS)], effectiveness (e.g., proportion of seizure clusters requiring only one dose), and safety profiles. In clinical studies, the proportion of seizure clusters for which only one dose of medication was used varied between the three approved rescue therapies with the highest single-dose rate for any time period for DNS; however, although studies for all three preparations enrolled patients with highly intractable epilepsy, inclusion and exclusion criteria varied, so the three cannot be directly compared. Treatments that have been used off-label for seizure clusters in the USA include midazolam for injection as an intranasal spray (indicated for sedation/anxiolysis/amnesia and anesthesia) and tablet forms of clonazepam (indicated for treatment for seizure disorders) and lorazepam (indicated for anxiety). In the European Union, buccal and intranasal midazolam are used for treating the indication of prolonged, acute convulsive seizures and rectal diazepam solution for the indication of epileptic and febrile convulsions; duration of effectiveness for these medications for the treatment of seizure clusters has not been established. This paper examines the literature context for understanding seizure clusters and their treatment and provides effectiveness, safety, and administration details for the three FDA-approved rescue therapies. Additionally, other medications that are used for rescue therapy in the USA and globally are discussed. Finally, the potential benefits of seizure action plans and candidates for their use are addressed. This paper is intended to provide details about the unique characteristics of rescue therapies for seizure clusters to help clarify appropriate treatment for individual patients.</p>","PeriodicalId":10508,"journal":{"name":"CNS drugs","volume":" ","pages":"125-140"},"PeriodicalIF":7.4000,"publicationDate":"2024-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10881644/pdf/","citationCount":"0","resultStr":"{\"title\":\"Benzodiazepines for the Treatment of Seizure Clusters.\",\"authors\":\"Patricia E Penovich, Vikram R Rao, Lucretia Long, Enrique Carrazana, Adrian L Rabinowicz\",\"doi\":\"10.1007/s40263-023-01060-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Patients with epilepsy may experience seizure clusters, which are described by the US Food and Drug Administration (FDA) as intermittent, stereotypic episodes of frequent seizure activity that are distinct from a patient's usual seizure pattern. Untreated seizure clusters may increase the risk for status epilepticus, as well as decrease quality of life and increase burden on patients and care partners. Benzodiazepine therapies are the mainstay for acute treatment of seizure clusters and are often administered by nonmedical care partners outside a healthcare facility. Three rescue therapies are currently FDA-approved for this indication, with diazepam rectal gel being the first in 1997, for patients aged ≥ 2 years. Limitations of rectal administration (e.g., positioning and disrobing the patient, which may affect ease of use and social acceptability; interpatient variation in bioavailability) led to the investigation of the potential for nasal administration as an alternative. Midazolam nasal spray (MDS) was approved by the FDA in 2019 for patients aged ≥ 12 years and diazepam nasal spray (DNS) in 2020 for patients aged ≥ 6 years; these two intranasal therapies have differences in their formulations [e.g., organic solvents (MDS) vs. Intravail and vitamin E for absorption and solubility (DNS)], effectiveness (e.g., proportion of seizure clusters requiring only one dose), and safety profiles. In clinical studies, the proportion of seizure clusters for which only one dose of medication was used varied between the three approved rescue therapies with the highest single-dose rate for any time period for DNS; however, although studies for all three preparations enrolled patients with highly intractable epilepsy, inclusion and exclusion criteria varied, so the three cannot be directly compared. Treatments that have been used off-label for seizure clusters in the USA include midazolam for injection as an intranasal spray (indicated for sedation/anxiolysis/amnesia and anesthesia) and tablet forms of clonazepam (indicated for treatment for seizure disorders) and lorazepam (indicated for anxiety). In the European Union, buccal and intranasal midazolam are used for treating the indication of prolonged, acute convulsive seizures and rectal diazepam solution for the indication of epileptic and febrile convulsions; duration of effectiveness for these medications for the treatment of seizure clusters has not been established. This paper examines the literature context for understanding seizure clusters and their treatment and provides effectiveness, safety, and administration details for the three FDA-approved rescue therapies. Additionally, other medications that are used for rescue therapy in the USA and globally are discussed. Finally, the potential benefits of seizure action plans and candidates for their use are addressed. This paper is intended to provide details about the unique characteristics of rescue therapies for seizure clusters to help clarify appropriate treatment for individual patients.</p>\",\"PeriodicalId\":10508,\"journal\":{\"name\":\"CNS drugs\",\"volume\":\" \",\"pages\":\"125-140\"},\"PeriodicalIF\":7.4000,\"publicationDate\":\"2024-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10881644/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"CNS drugs\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s40263-023-01060-1\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/2/15 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"CNS drugs","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40263-023-01060-1","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/15 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
癫痫患者可能会出现发作群,美国食品药品管理局(FDA)将其描述为频繁发作活动的间歇性、刻板性发作,与患者通常的发作模式截然不同。未经治疗的癫痫发作群可能会增加癫痫状态的风险,降低生活质量,增加患者和护理伙伴的负担。苯二氮卓类药物是急性治疗癫痫发作群集的主要药物,通常由医疗机构以外的非医疗护理伙伴使用。目前,美国食品及药物管理局批准了三种用于这一适应症的抢救疗法,其中地西泮直肠凝胶是 1997 年批准的第一种疗法,适用于年龄≥ 2 岁的患者。直肠给药的局限性(例如,需要让患者就位和脱衣,这可能会影响使用的方便性和社会接受度;患者之间生物利用度的差异)促使人们开始研究鼻腔给药作为替代品的可能性。美国食品和药物管理局于 2019 年批准咪达唑仑鼻腔喷雾剂(MDS)用于年龄≥12 岁的患者,并于 2020 年批准地西泮鼻腔喷雾剂(DNS)用于年龄≥6 岁的患者;这两种鼻内疗法在配方[如有机溶剂(MDS)与促进吸收和溶解的 Intravail 和维生素 E(DNS)]、有效性(如只需一次给药的癫痫发作群比例)和安全性方面存在差异。在临床研究中,三种获批的抢救疗法只需使用一剂药物的发作群比例各不相同,其中 DNS 在任何时间段内的单剂使用率最高;不过,虽然所有三种制剂的研究都招募了高度难治性癫痫患者,但纳入和排除标准各不相同,因此无法对这三种制剂进行直接比较。在美国,标签外用于治疗癫痫发作群的药物包括米达唑仑鼻内喷雾注射剂(适用于镇静/抗焦虑/失眠和麻醉)以及氯硝西泮片剂(适用于治疗癫痫发作紊乱)和劳拉西泮片剂(适用于治疗焦虑)。在欧盟,口腔和鼻内咪达唑仑用于治疗长期急性惊厥发作,直肠地西泮溶液用于治疗癫痫和发热性惊厥;这些药物治疗癫痫发作群的有效期尚未确定。本文研究了了解癫痫发作群及其治疗的文献背景,并提供了三种经 FDA 批准的抢救疗法的有效性、安全性和用药详情。此外,本文还讨论了在美国和全球范围内用于抢救治疗的其他药物。最后,还讨论了癫痫发作行动计划的潜在益处及其使用人选。本文旨在详细介绍针对癫痫发作群的抢救疗法的独特性,以帮助明确针对个别患者的适当治疗方法。
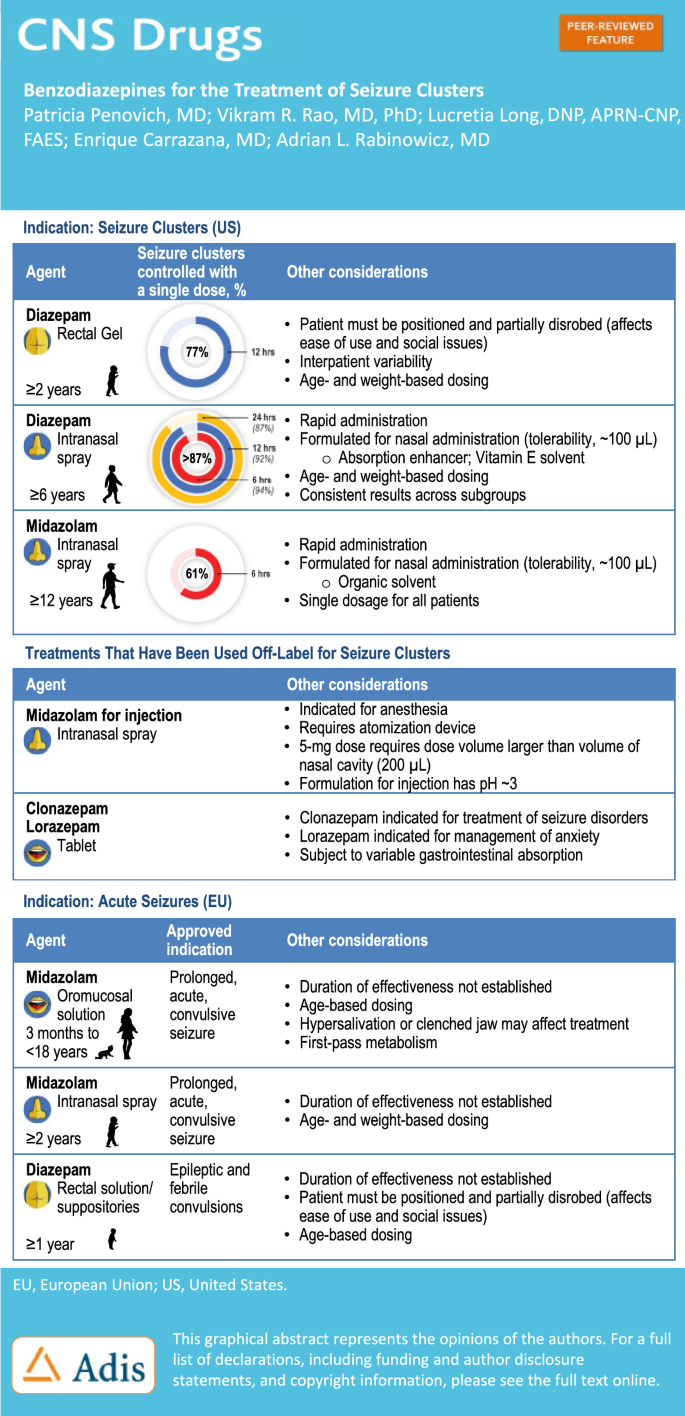
Benzodiazepines for the Treatment of Seizure Clusters.
Patients with epilepsy may experience seizure clusters, which are described by the US Food and Drug Administration (FDA) as intermittent, stereotypic episodes of frequent seizure activity that are distinct from a patient's usual seizure pattern. Untreated seizure clusters may increase the risk for status epilepticus, as well as decrease quality of life and increase burden on patients and care partners. Benzodiazepine therapies are the mainstay for acute treatment of seizure clusters and are often administered by nonmedical care partners outside a healthcare facility. Three rescue therapies are currently FDA-approved for this indication, with diazepam rectal gel being the first in 1997, for patients aged ≥ 2 years. Limitations of rectal administration (e.g., positioning and disrobing the patient, which may affect ease of use and social acceptability; interpatient variation in bioavailability) led to the investigation of the potential for nasal administration as an alternative. Midazolam nasal spray (MDS) was approved by the FDA in 2019 for patients aged ≥ 12 years and diazepam nasal spray (DNS) in 2020 for patients aged ≥ 6 years; these two intranasal therapies have differences in their formulations [e.g., organic solvents (MDS) vs. Intravail and vitamin E for absorption and solubility (DNS)], effectiveness (e.g., proportion of seizure clusters requiring only one dose), and safety profiles. In clinical studies, the proportion of seizure clusters for which only one dose of medication was used varied between the three approved rescue therapies with the highest single-dose rate for any time period for DNS; however, although studies for all three preparations enrolled patients with highly intractable epilepsy, inclusion and exclusion criteria varied, so the three cannot be directly compared. Treatments that have been used off-label for seizure clusters in the USA include midazolam for injection as an intranasal spray (indicated for sedation/anxiolysis/amnesia and anesthesia) and tablet forms of clonazepam (indicated for treatment for seizure disorders) and lorazepam (indicated for anxiety). In the European Union, buccal and intranasal midazolam are used for treating the indication of prolonged, acute convulsive seizures and rectal diazepam solution for the indication of epileptic and febrile convulsions; duration of effectiveness for these medications for the treatment of seizure clusters has not been established. This paper examines the literature context for understanding seizure clusters and their treatment and provides effectiveness, safety, and administration details for the three FDA-approved rescue therapies. Additionally, other medications that are used for rescue therapy in the USA and globally are discussed. Finally, the potential benefits of seizure action plans and candidates for their use are addressed. This paper is intended to provide details about the unique characteristics of rescue therapies for seizure clusters to help clarify appropriate treatment for individual patients.
期刊介绍:
CNS Drugs promotes rational pharmacotherapy within the disciplines of clinical psychiatry and neurology. The Journal includes:
- Overviews of contentious or emerging issues.
- Comprehensive narrative reviews that provide an authoritative source of information on pharmacological approaches to managing neurological and psychiatric illnesses.
- Systematic reviews that collate empirical evidence to answer a specific research question, using explicit, systematic methods as outlined by the PRISMA statement.
- Adis Drug Reviews of the properties and place in therapy of both newer and established drugs in neurology and psychiatry.
- Original research articles reporting the results of well-designed studies with a strong link to clinical practice, such as clinical pharmacodynamic and pharmacokinetic studies, clinical trials, meta-analyses, outcomes research, and pharmacoeconomic and pharmacoepidemiological studies.
Additional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in CNS Drugs may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand important medical advances.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
