Ralph Pruijsten, Gerrie Prins-van Gilst, Chantal Schuiling, Monique van Dijk, Marc Schluep
{"title":"过渡到单人病房是否会影响院内心脏骤停的发生率和结果?","authors":"Ralph Pruijsten, Gerrie Prins-van Gilst, Chantal Schuiling, Monique van Dijk, Marc Schluep","doi":"10.1177/19375867241226600","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>It is proposed that patients in single-occupancy patient rooms (SPRs) carry a risk of less surveillance by nursing and medical staff and that resuscitation teams need longer to arrive in case of in-hospital cardiac arrest (IHCA). Higher incidences of IHCA and worse outcomes after cardiopulmonary resuscitation (CPR) may be the result.</p><p><strong>Objectives: </strong>Our study examines whether there is a difference in incidence and outcomes of IHCA before and after the transition from a hospital with multibedded rooms to solely SPRs.</p><p><strong>Methods: </strong>In this prospective observational study in a Dutch university hospital, as a part of the Resuscitation Outcomes in the Netherlands study, we reviewed all cases of IHCA on general adult wards in a period of 16.5 months before to 16.5 months after the transition to SPRs.</p><p><strong>Results: </strong>During the study period, 102 CPR attempts were performed: 51 in the former hospital and 51 in the new hospital. Median time between last-seen-well and start basic life support did not differ significantly, nor did median time to arrival of the CPR team. Survival rates to hospital discharge were 30.0% versus 29.4% of resuscitated patients (<i>p</i> = 1.00), with comparable neurological outcomes: 86.7% of discharged patients in the new hospital had Cerebral Performance Category 1 (good cerebral performance) versus 46.7% in the former hospital (<i>p</i> = .067). When corrected for telemetry monitoring, these differences were still nonsignificant.</p><p><strong>Conclusions: </strong>The transition to a 100% SPR hospital had no negative impact on incidence, survival rates, and neurological outcomes of IHCAs on general adult wards.</p>","PeriodicalId":47306,"journal":{"name":"Herd-Health Environments Research & Design Journal","volume":" ","pages":"68-76"},"PeriodicalIF":1.8000,"publicationDate":"2024-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11468116/pdf/","citationCount":"0","resultStr":"{\"title\":\"Does a Transition to Single-Occupancy Patient Rooms Affect the Incidence and Outcome of In-Hospital Cardiac Arrests?\",\"authors\":\"Ralph Pruijsten, Gerrie Prins-van Gilst, Chantal Schuiling, Monique van Dijk, Marc Schluep\",\"doi\":\"10.1177/19375867241226600\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>It is proposed that patients in single-occupancy patient rooms (SPRs) carry a risk of less surveillance by nursing and medical staff and that resuscitation teams need longer to arrive in case of in-hospital cardiac arrest (IHCA). Higher incidences of IHCA and worse outcomes after cardiopulmonary resuscitation (CPR) may be the result.</p><p><strong>Objectives: </strong>Our study examines whether there is a difference in incidence and outcomes of IHCA before and after the transition from a hospital with multibedded rooms to solely SPRs.</p><p><strong>Methods: </strong>In this prospective observational study in a Dutch university hospital, as a part of the Resuscitation Outcomes in the Netherlands study, we reviewed all cases of IHCA on general adult wards in a period of 16.5 months before to 16.5 months after the transition to SPRs.</p><p><strong>Results: </strong>During the study period, 102 CPR attempts were performed: 51 in the former hospital and 51 in the new hospital. Median time between last-seen-well and start basic life support did not differ significantly, nor did median time to arrival of the CPR team. Survival rates to hospital discharge were 30.0% versus 29.4% of resuscitated patients (<i>p</i> = 1.00), with comparable neurological outcomes: 86.7% of discharged patients in the new hospital had Cerebral Performance Category 1 (good cerebral performance) versus 46.7% in the former hospital (<i>p</i> = .067). When corrected for telemetry monitoring, these differences were still nonsignificant.</p><p><strong>Conclusions: </strong>The transition to a 100% SPR hospital had no negative impact on incidence, survival rates, and neurological outcomes of IHCAs on general adult wards.</p>\",\"PeriodicalId\":47306,\"journal\":{\"name\":\"Herd-Health Environments Research & Design Journal\",\"volume\":\" \",\"pages\":\"68-76\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2024-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11468116/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Herd-Health Environments Research & Design Journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/19375867241226600\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/2/23 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Herd-Health Environments Research & Design Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/19375867241226600","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/2/23 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
Does a Transition to Single-Occupancy Patient Rooms Affect the Incidence and Outcome of In-Hospital Cardiac Arrests?
Background: It is proposed that patients in single-occupancy patient rooms (SPRs) carry a risk of less surveillance by nursing and medical staff and that resuscitation teams need longer to arrive in case of in-hospital cardiac arrest (IHCA). Higher incidences of IHCA and worse outcomes after cardiopulmonary resuscitation (CPR) may be the result.
Objectives: Our study examines whether there is a difference in incidence and outcomes of IHCA before and after the transition from a hospital with multibedded rooms to solely SPRs.
Methods: In this prospective observational study in a Dutch university hospital, as a part of the Resuscitation Outcomes in the Netherlands study, we reviewed all cases of IHCA on general adult wards in a period of 16.5 months before to 16.5 months after the transition to SPRs.
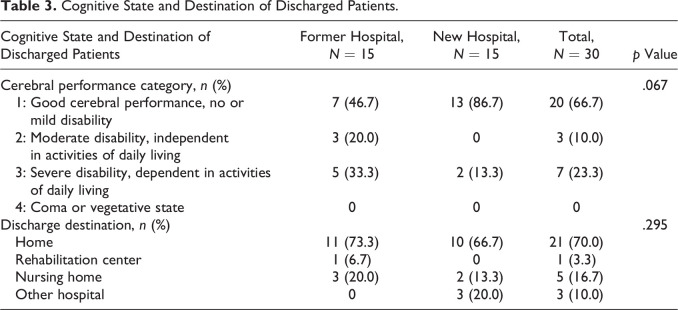
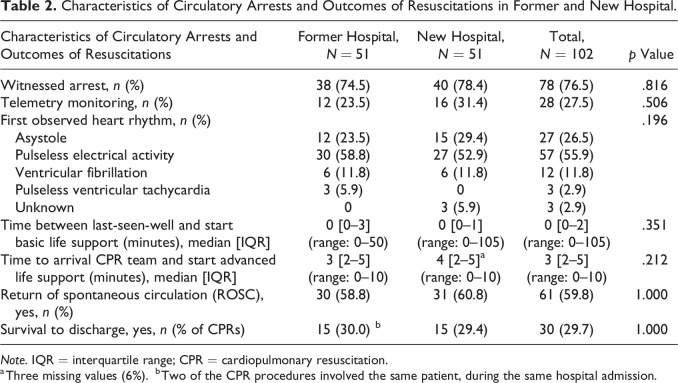
Results: During the study period, 102 CPR attempts were performed: 51 in the former hospital and 51 in the new hospital. Median time between last-seen-well and start basic life support did not differ significantly, nor did median time to arrival of the CPR team. Survival rates to hospital discharge were 30.0% versus 29.4% of resuscitated patients (p = 1.00), with comparable neurological outcomes: 86.7% of discharged patients in the new hospital had Cerebral Performance Category 1 (good cerebral performance) versus 46.7% in the former hospital (p = .067). When corrected for telemetry monitoring, these differences were still nonsignificant.
Conclusions: The transition to a 100% SPR hospital had no negative impact on incidence, survival rates, and neurological outcomes of IHCAs on general adult wards.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
