Steven Markowitz MD, DrPH, Knut Ringen DrPH, MHA, MPH, John M. Dement PhD, Kurt Straif MD, PhD, MPH, L. Christine Oliver MD, MPH, MS, Eduardo Algranti MD, MSc, PhD, Dennis Nowak MD, Rodney Ehrlich MBCHB, DOH, FCPHM(SA)(Occ Med), PhD, Melissa A. McDiarmid MD, MPH, DABT, Albert Miller MD, Collegium Ramazzini
{"title":"职业性肺癌筛查:拉马齐尼学院声明。","authors":"Steven Markowitz MD, DrPH, Knut Ringen DrPH, MHA, MPH, John M. Dement PhD, Kurt Straif MD, PhD, MPH, L. Christine Oliver MD, MPH, MS, Eduardo Algranti MD, MSc, PhD, Dennis Nowak MD, Rodney Ehrlich MBCHB, DOH, FCPHM(SA)(Occ Med), PhD, Melissa A. McDiarmid MD, MPH, DABT, Albert Miller MD, Collegium Ramazzini","doi":"10.1002/ajim.23572","DOIUrl":null,"url":null,"abstract":"<p>Lung cancer is the most common cause of death from cancer in the world. It is also the most common lethal work-related cancer. After tobacco smoking, occupational exposures present the most frequent specific cause of lung cancer that is amenable to intervention.</p><p>Early detection and treatment can identify and cure primary lung cancer. Randomized controlled trials have demonstrated the efficacy of low dose computed tomography (LDCT) screening among persons at high risk of lung cancer. Guidelines for determining eligibility for LDCT screening have been established for the general population but have largely neglected those for whom occupational exposure to lung carcinogens is a risk factor.</p><p>The Collegium recommends that persons at risk for lung cancer from occupational exposures be offered annual LDCT if their cumulative risk of lung cancer approximates the level of risk endorsed by the guidelines promulgated by the United States Preventive Services Task Force (USPSTF) in 2021 and the National Comprehensive Cancer Network (NCCN) in the United States in 2021. At present, these agencies recommend screening for people aged 50 and over who have smoked at least 20 pack-years of cigarettes. The Collegium recommends that additional lung cancer risk factors, including exposure to known or suspected occupational and environmental lung carcinogens; family history of lung cancer (especially among first degree relatives and relatives <60 years of age); a personal history of chronic obstructive lung disease, pneumoconiosis, or pulmonary fibrosis; or a personal history of cancer (excluding skin cancer) be considered as part of the risk assessment for eligibility determination for lung cancer screening. Latency, or the period of time since initial occupational exposure (e.g., >15 years) is another factor that should be considered. If the presence of these additional risk factors, in combination with age and smoking history, is associated with a level of risk that meets or exceeds the level of risk identified by the USPSTF and NCCN, then an annual low dose chest CT for lung cancer screening should be offered. We do not favor a specific age cut-off at which to end screening, but we recognize that only persons who are sufficiently healthy and have sufficient life expectancy to undergo diagnostic work-up and potentially curative treatment should be offered screening for lung cancer. In view of the rising risk of occupational lung cancer over time and the potential or actual interaction between occupational lung carcinogens and cigarette smoking even after quitting, screening programs may choose to screen workers with occupational lung cancer risk for prolonged periods after they have quit smoking cigarettes. The Collegium acknowledges that there are uncertainties and assumptions entailed in this approach and that risk assessment for individual workers necessitates application of significant professional judgement. We encourage the implementation of well-organized screening programs that can further our knowledge about optimal occupation-inclusive lung cancer screening strategies.</p><p>Workers with a history of exposure to known or suspected lung carcinogens or working in occupations/trades or work tasks that are known to elevate the risk for lung cancer form the target population for lung cancer screening. Important examples of lung carcinogens include asbestos, silica, diesel exhaust, welding fumes, selected metals, and radiation.</p><p>The Collegium calls upon occupational health and medical professionals and stakeholders (governments, employers, insurance companies, and labor unions) to identify worker populations that have excess lung cancer risk, to promote lung cancer screening, and to develop and support well-organized programs to conduct such screening in these populations.</p><p>While elimination or minimization of exposure to lung carcinogens in the workplace through environmental controls is critical for lung cancer prevention, lung cancer screening is an essential secondary intervention for reducing deaths and disabling disease from exposure to workplace lung carcinogens.</p><p>Steven Markowitz, Knut Ringen, and John M. Dement conceived the work and wrote the first draft. All authors edited the Statement and added intellectual contributions. All authors have approved this manuscript version for submission and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The Collegium Ramazzini conducted peer review of the Statement and its membership approved the final Statement.</p><p>The Collegium Ramazzini is an international scientific society that examines critical issues in occupational and environmental medicine with a view towards action to prevent disease and promote health. The Collegium derives its name from Bernardino Ramazzini, the father of occupational medicine, a professor of medicine of the Universities of Modena and Padua in the late 1600s and the early 1700s. The Collegium is comprised of 180 physicians and scientists from 35 countries, each of whom is elected to membership. The Collegium is independent of commercial interests.</p><p>Dr. Steven Markowitz has a financial assistance agreement with the U.S. Department of Energy (DOE) to screen DOE workers for lung cancer using low dose chest CT scans. Drs. Knut Ringen and John Dement have a financial assistance agreement with the U.S. Department of Energy (DOE) to screen DOE construction workers for lung cancer using low dose chest CT scans. Dr. Dennis Nowak is a member of an advisory board of Pfizer Inc. regarding reimbursement of varenicline for smoking cessation. Dr. Nowak provides clinical, pharmacological, and psychological support for nicotine abstinence in smokers and high risk workers. The remaining authors declare no conflict of interest.</p><p>John Meyer declares that he has no conflict of interest in the review and publication decision regarding this article.</p>","PeriodicalId":7873,"journal":{"name":"American journal of industrial medicine","volume":"67 4","pages":"289-303"},"PeriodicalIF":3.1000,"publicationDate":"2024-03-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ajim.23572","citationCount":"0","resultStr":"{\"title\":\"Occupational lung cancer screening: A Collegium Ramazzini statement\",\"authors\":\"Steven Markowitz MD, DrPH, Knut Ringen DrPH, MHA, MPH, John M. Dement PhD, Kurt Straif MD, PhD, MPH, L. Christine Oliver MD, MPH, MS, Eduardo Algranti MD, MSc, PhD, Dennis Nowak MD, Rodney Ehrlich MBCHB, DOH, FCPHM(SA)(Occ Med), PhD, Melissa A. McDiarmid MD, MPH, DABT, Albert Miller MD, Collegium Ramazzini\",\"doi\":\"10.1002/ajim.23572\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Lung cancer is the most common cause of death from cancer in the world. It is also the most common lethal work-related cancer. After tobacco smoking, occupational exposures present the most frequent specific cause of lung cancer that is amenable to intervention.</p><p>Early detection and treatment can identify and cure primary lung cancer. Randomized controlled trials have demonstrated the efficacy of low dose computed tomography (LDCT) screening among persons at high risk of lung cancer. Guidelines for determining eligibility for LDCT screening have been established for the general population but have largely neglected those for whom occupational exposure to lung carcinogens is a risk factor.</p><p>The Collegium recommends that persons at risk for lung cancer from occupational exposures be offered annual LDCT if their cumulative risk of lung cancer approximates the level of risk endorsed by the guidelines promulgated by the United States Preventive Services Task Force (USPSTF) in 2021 and the National Comprehensive Cancer Network (NCCN) in the United States in 2021. At present, these agencies recommend screening for people aged 50 and over who have smoked at least 20 pack-years of cigarettes. The Collegium recommends that additional lung cancer risk factors, including exposure to known or suspected occupational and environmental lung carcinogens; family history of lung cancer (especially among first degree relatives and relatives <60 years of age); a personal history of chronic obstructive lung disease, pneumoconiosis, or pulmonary fibrosis; or a personal history of cancer (excluding skin cancer) be considered as part of the risk assessment for eligibility determination for lung cancer screening. Latency, or the period of time since initial occupational exposure (e.g., >15 years) is another factor that should be considered. If the presence of these additional risk factors, in combination with age and smoking history, is associated with a level of risk that meets or exceeds the level of risk identified by the USPSTF and NCCN, then an annual low dose chest CT for lung cancer screening should be offered. We do not favor a specific age cut-off at which to end screening, but we recognize that only persons who are sufficiently healthy and have sufficient life expectancy to undergo diagnostic work-up and potentially curative treatment should be offered screening for lung cancer. In view of the rising risk of occupational lung cancer over time and the potential or actual interaction between occupational lung carcinogens and cigarette smoking even after quitting, screening programs may choose to screen workers with occupational lung cancer risk for prolonged periods after they have quit smoking cigarettes. The Collegium acknowledges that there are uncertainties and assumptions entailed in this approach and that risk assessment for individual workers necessitates application of significant professional judgement. We encourage the implementation of well-organized screening programs that can further our knowledge about optimal occupation-inclusive lung cancer screening strategies.</p><p>Workers with a history of exposure to known or suspected lung carcinogens or working in occupations/trades or work tasks that are known to elevate the risk for lung cancer form the target population for lung cancer screening. Important examples of lung carcinogens include asbestos, silica, diesel exhaust, welding fumes, selected metals, and radiation.</p><p>The Collegium calls upon occupational health and medical professionals and stakeholders (governments, employers, insurance companies, and labor unions) to identify worker populations that have excess lung cancer risk, to promote lung cancer screening, and to develop and support well-organized programs to conduct such screening in these populations.</p><p>While elimination or minimization of exposure to lung carcinogens in the workplace through environmental controls is critical for lung cancer prevention, lung cancer screening is an essential secondary intervention for reducing deaths and disabling disease from exposure to workplace lung carcinogens.</p><p>Steven Markowitz, Knut Ringen, and John M. Dement conceived the work and wrote the first draft. All authors edited the Statement and added intellectual contributions. All authors have approved this manuscript version for submission and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The Collegium Ramazzini conducted peer review of the Statement and its membership approved the final Statement.</p><p>The Collegium Ramazzini is an international scientific society that examines critical issues in occupational and environmental medicine with a view towards action to prevent disease and promote health. The Collegium derives its name from Bernardino Ramazzini, the father of occupational medicine, a professor of medicine of the Universities of Modena and Padua in the late 1600s and the early 1700s. The Collegium is comprised of 180 physicians and scientists from 35 countries, each of whom is elected to membership. The Collegium is independent of commercial interests.</p><p>Dr. Steven Markowitz has a financial assistance agreement with the U.S. Department of Energy (DOE) to screen DOE workers for lung cancer using low dose chest CT scans. Drs. Knut Ringen and John Dement have a financial assistance agreement with the U.S. Department of Energy (DOE) to screen DOE construction workers for lung cancer using low dose chest CT scans. Dr. Dennis Nowak is a member of an advisory board of Pfizer Inc. regarding reimbursement of varenicline for smoking cessation. Dr. Nowak provides clinical, pharmacological, and psychological support for nicotine abstinence in smokers and high risk workers. The remaining authors declare no conflict of interest.</p><p>John Meyer declares that he has no conflict of interest in the review and publication decision regarding this article.</p>\",\"PeriodicalId\":7873,\"journal\":{\"name\":\"American journal of industrial medicine\",\"volume\":\"67 4\",\"pages\":\"289-303\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2024-03-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ajim.23572\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"American journal of industrial medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ajim.23572\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"American journal of industrial medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ajim.23572","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
Occupational lung cancer screening: A Collegium Ramazzini statement
Lung cancer is the most common cause of death from cancer in the world. It is also the most common lethal work-related cancer. After tobacco smoking, occupational exposures present the most frequent specific cause of lung cancer that is amenable to intervention.
Early detection and treatment can identify and cure primary lung cancer. Randomized controlled trials have demonstrated the efficacy of low dose computed tomography (LDCT) screening among persons at high risk of lung cancer. Guidelines for determining eligibility for LDCT screening have been established for the general population but have largely neglected those for whom occupational exposure to lung carcinogens is a risk factor.
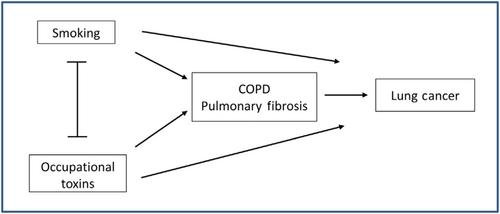
The Collegium recommends that persons at risk for lung cancer from occupational exposures be offered annual LDCT if their cumulative risk of lung cancer approximates the level of risk endorsed by the guidelines promulgated by the United States Preventive Services Task Force (USPSTF) in 2021 and the National Comprehensive Cancer Network (NCCN) in the United States in 2021. At present, these agencies recommend screening for people aged 50 and over who have smoked at least 20 pack-years of cigarettes. The Collegium recommends that additional lung cancer risk factors, including exposure to known or suspected occupational and environmental lung carcinogens; family history of lung cancer (especially among first degree relatives and relatives <60 years of age); a personal history of chronic obstructive lung disease, pneumoconiosis, or pulmonary fibrosis; or a personal history of cancer (excluding skin cancer) be considered as part of the risk assessment for eligibility determination for lung cancer screening. Latency, or the period of time since initial occupational exposure (e.g., >15 years) is another factor that should be considered. If the presence of these additional risk factors, in combination with age and smoking history, is associated with a level of risk that meets or exceeds the level of risk identified by the USPSTF and NCCN, then an annual low dose chest CT for lung cancer screening should be offered. We do not favor a specific age cut-off at which to end screening, but we recognize that only persons who are sufficiently healthy and have sufficient life expectancy to undergo diagnostic work-up and potentially curative treatment should be offered screening for lung cancer. In view of the rising risk of occupational lung cancer over time and the potential or actual interaction between occupational lung carcinogens and cigarette smoking even after quitting, screening programs may choose to screen workers with occupational lung cancer risk for prolonged periods after they have quit smoking cigarettes. The Collegium acknowledges that there are uncertainties and assumptions entailed in this approach and that risk assessment for individual workers necessitates application of significant professional judgement. We encourage the implementation of well-organized screening programs that can further our knowledge about optimal occupation-inclusive lung cancer screening strategies.
Workers with a history of exposure to known or suspected lung carcinogens or working in occupations/trades or work tasks that are known to elevate the risk for lung cancer form the target population for lung cancer screening. Important examples of lung carcinogens include asbestos, silica, diesel exhaust, welding fumes, selected metals, and radiation.
The Collegium calls upon occupational health and medical professionals and stakeholders (governments, employers, insurance companies, and labor unions) to identify worker populations that have excess lung cancer risk, to promote lung cancer screening, and to develop and support well-organized programs to conduct such screening in these populations.
While elimination or minimization of exposure to lung carcinogens in the workplace through environmental controls is critical for lung cancer prevention, lung cancer screening is an essential secondary intervention for reducing deaths and disabling disease from exposure to workplace lung carcinogens.
Steven Markowitz, Knut Ringen, and John M. Dement conceived the work and wrote the first draft. All authors edited the Statement and added intellectual contributions. All authors have approved this manuscript version for submission and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The Collegium Ramazzini conducted peer review of the Statement and its membership approved the final Statement.
The Collegium Ramazzini is an international scientific society that examines critical issues in occupational and environmental medicine with a view towards action to prevent disease and promote health. The Collegium derives its name from Bernardino Ramazzini, the father of occupational medicine, a professor of medicine of the Universities of Modena and Padua in the late 1600s and the early 1700s. The Collegium is comprised of 180 physicians and scientists from 35 countries, each of whom is elected to membership. The Collegium is independent of commercial interests.
Dr. Steven Markowitz has a financial assistance agreement with the U.S. Department of Energy (DOE) to screen DOE workers for lung cancer using low dose chest CT scans. Drs. Knut Ringen and John Dement have a financial assistance agreement with the U.S. Department of Energy (DOE) to screen DOE construction workers for lung cancer using low dose chest CT scans. Dr. Dennis Nowak is a member of an advisory board of Pfizer Inc. regarding reimbursement of varenicline for smoking cessation. Dr. Nowak provides clinical, pharmacological, and psychological support for nicotine abstinence in smokers and high risk workers. The remaining authors declare no conflict of interest.
John Meyer declares that he has no conflict of interest in the review and publication decision regarding this article.
期刊介绍:
American Journal of Industrial Medicine considers for publication reports of original research, review articles, instructive case reports, and analyses of policy in the fields of occupational and environmental health and safety. The Journal also accepts commentaries, book reviews and letters of comment and criticism. The goals of the journal are to advance and disseminate knowledge, promote research and foster the prevention of disease and injury. Specific topics of interest include: occupational disease; environmental disease; pesticides; cancer; occupational epidemiology; environmental epidemiology; disease surveillance systems; ergonomics; dust diseases; lead poisoning; neurotoxicology; endocrine disruptors.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
