Kate Curtis RN, PhD, Benjamin Clark BSc (Adv), MChD, Mary K Lam BA (Hons), MHIM, PhD, Ryan Huckle BMBS, BA (Hons), Geoffrey Melville BASc (Hons), PhD, Simon Binks BMedSci, BM, BS, FRCEM, FACEM, Ms Wende Ryan RN, Trevor Gardner OAM, BSc (Hons), MBBS, Ms Brooke Parsons RN, RM, GCert Emerg Nursing, Bruce Ashford BDSc (Hons), MBBS, PhD, FRACS
{"title":"反思分级创伤团队响应:地区创伤中心的病例系列研究。","authors":"Kate Curtis RN, PhD, Benjamin Clark BSc (Adv), MChD, Mary K Lam BA (Hons), MHIM, PhD, Ryan Huckle BMBS, BA (Hons), Geoffrey Melville BASc (Hons), PhD, Simon Binks BMedSci, BM, BS, FRCEM, FACEM, Ms Wende Ryan RN, Trevor Gardner OAM, BSc (Hons), MBBS, Ms Brooke Parsons RN, RM, GCert Emerg Nursing, Bruce Ashford BDSc (Hons), MBBS, PhD, FRACS","doi":"10.1111/1742-6723.14399","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Objective</h3>\n \n <p>To reduce perceived unnecessary resource use, we modified our tiered trauma response. If a patient was not physiologically compromised, surgical registrar attendance was not mandated. We investigated the effect of this change on missed injury, unplanned representation to ED, diagnostic imaging rates and staff satisfaction.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>A retrospective case series study assessing the 3-month period before and after the intervention was conducted. Logistic regression analyses were used to examine the association between ordering of computerised tomography (CT) and ED length of stay (LOS), injury severity (ISS), age, surgical review and admission. A staff survey was conducted to investigate staff perceptions of the practice change. Free text data were analysed using inductive content analysis.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>There were 105 patients in the control and 166 in the intervention group and their mean (SD) ISS was the same (ISS [SD] = 4 [±4] [<i>P</i> = 0.608]). A higher proportion of the control group were admitted (56.3% <i>vs</i> 42.2% [<i>P</i> = 0.032]) and they had a shorter ED LOS (274 min [202–456] <i>vs</i> 326 min [225–560], <i>P</i> = 0.044). The rate of missed injury was unchanged. A surgical review resulted in a 26-fold increase in receipt of a whole-body CT scan (odds ratio = 26.89, 95% confidence interval = 3.31–218.17). Just over half of survey respondents felt the change was safe (54.4%), and more surgical (90%) than ED staff (69%) reported the change as positive.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>The removal of the surgical registrar from the initial trauma standby response did not result in any adverse events, reduced admissions, pathology and imaging, but resulted in an increased ED LOS and time to surgical review.</p>\n </section>\n </div>","PeriodicalId":11604,"journal":{"name":"Emergency Medicine Australasia","volume":"36 4","pages":"571-578"},"PeriodicalIF":1.4000,"publicationDate":"2024-03-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/1742-6723.14399","citationCount":"0","resultStr":"{\"title\":\"Rethinking the tiered trauma team response: A case-series study in a regional trauma centre\",\"authors\":\"Kate Curtis RN, PhD, Benjamin Clark BSc (Adv), MChD, Mary K Lam BA (Hons), MHIM, PhD, Ryan Huckle BMBS, BA (Hons), Geoffrey Melville BASc (Hons), PhD, Simon Binks BMedSci, BM, BS, FRCEM, FACEM, Ms Wende Ryan RN, Trevor Gardner OAM, BSc (Hons), MBBS, Ms Brooke Parsons RN, RM, GCert Emerg Nursing, Bruce Ashford BDSc (Hons), MBBS, PhD, FRACS\",\"doi\":\"10.1111/1742-6723.14399\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Objective</h3>\\n \\n <p>To reduce perceived unnecessary resource use, we modified our tiered trauma response. If a patient was not physiologically compromised, surgical registrar attendance was not mandated. We investigated the effect of this change on missed injury, unplanned representation to ED, diagnostic imaging rates and staff satisfaction.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>A retrospective case series study assessing the 3-month period before and after the intervention was conducted. Logistic regression analyses were used to examine the association between ordering of computerised tomography (CT) and ED length of stay (LOS), injury severity (ISS), age, surgical review and admission. A staff survey was conducted to investigate staff perceptions of the practice change. Free text data were analysed using inductive content analysis.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>There were 105 patients in the control and 166 in the intervention group and their mean (SD) ISS was the same (ISS [SD] = 4 [±4] [<i>P</i> = 0.608]). A higher proportion of the control group were admitted (56.3% <i>vs</i> 42.2% [<i>P</i> = 0.032]) and they had a shorter ED LOS (274 min [202–456] <i>vs</i> 326 min [225–560], <i>P</i> = 0.044). The rate of missed injury was unchanged. A surgical review resulted in a 26-fold increase in receipt of a whole-body CT scan (odds ratio = 26.89, 95% confidence interval = 3.31–218.17). Just over half of survey respondents felt the change was safe (54.4%), and more surgical (90%) than ED staff (69%) reported the change as positive.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>The removal of the surgical registrar from the initial trauma standby response did not result in any adverse events, reduced admissions, pathology and imaging, but resulted in an increased ED LOS and time to surgical review.</p>\\n </section>\\n </div>\",\"PeriodicalId\":11604,\"journal\":{\"name\":\"Emergency Medicine Australasia\",\"volume\":\"36 4\",\"pages\":\"571-578\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2024-03-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/1742-6723.14399\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Emergency Medicine Australasia\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/1742-6723.14399\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"EMERGENCY MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Emergency Medicine Australasia","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/1742-6723.14399","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
Rethinking the tiered trauma team response: A case-series study in a regional trauma centre
Objective
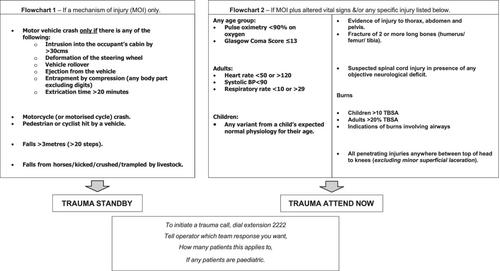
To reduce perceived unnecessary resource use, we modified our tiered trauma response. If a patient was not physiologically compromised, surgical registrar attendance was not mandated. We investigated the effect of this change on missed injury, unplanned representation to ED, diagnostic imaging rates and staff satisfaction.
Methods
A retrospective case series study assessing the 3-month period before and after the intervention was conducted. Logistic regression analyses were used to examine the association between ordering of computerised tomography (CT) and ED length of stay (LOS), injury severity (ISS), age, surgical review and admission. A staff survey was conducted to investigate staff perceptions of the practice change. Free text data were analysed using inductive content analysis.
Results
There were 105 patients in the control and 166 in the intervention group and their mean (SD) ISS was the same (ISS [SD] = 4 [±4] [P = 0.608]). A higher proportion of the control group were admitted (56.3% vs 42.2% [P = 0.032]) and they had a shorter ED LOS (274 min [202–456] vs 326 min [225–560], P = 0.044). The rate of missed injury was unchanged. A surgical review resulted in a 26-fold increase in receipt of a whole-body CT scan (odds ratio = 26.89, 95% confidence interval = 3.31–218.17). Just over half of survey respondents felt the change was safe (54.4%), and more surgical (90%) than ED staff (69%) reported the change as positive.
Conclusion
The removal of the surgical registrar from the initial trauma standby response did not result in any adverse events, reduced admissions, pathology and imaging, but resulted in an increased ED LOS and time to surgical review.
期刊介绍:
Emergency Medicine Australasia is the official journal of the Australasian College for Emergency Medicine (ACEM) and the Australasian Society for Emergency Medicine (ASEM), and publishes original articles dealing with all aspects of clinical practice, research, education and experiences in emergency medicine.
Original articles are published under the following sections: Original Research, Paediatric Emergency Medicine, Disaster Medicine, Education and Training, Ethics, International Emergency Medicine, Management and Quality, Medicolegal Matters, Prehospital Care, Public Health, Rural and Remote Care, Technology, Toxicology and Trauma. Accepted papers become the copyright of the journal.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
