Ling Li, Jannah Baker, Renee Quirk, Danielle Deidun, Maria Moran, Ahmed Abo Salem, Nanda Aryal, Bethany A Van Dort, Wu Yi Zheng, Andrew Hargreaves, Paula Doherty, Sarah N Hilmer, Richard O Day, Johanna I Westbrook, Melissa T Baysari
{"title":"药物间相互作用与对住院患者的实际伤害:一项多中心研究,探讨电子用药系统实施前后的普遍性。","authors":"Ling Li, Jannah Baker, Renee Quirk, Danielle Deidun, Maria Moran, Ahmed Abo Salem, Nanda Aryal, Bethany A Van Dort, Wu Yi Zheng, Andrew Hargreaves, Paula Doherty, Sarah N Hilmer, Richard O Day, Johanna I Westbrook, Melissa T Baysari","doi":"10.1007/s40264-024-01412-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Drug-drug interactions (DDIs) have potential to cause patient harm, including lowering therapeutic efficacy. This study aimed to (i) determine the prevalence of potential DDIs (pDDIs); clinically relevant DDIs (cDDIs), that is, DDIs that could lead to patient harm, taking into account a patient's individual clinical profile, drug effects and severity of potential harmful outcome; and subsequent actual harm among hospitalized patients and (ii) examine the impact of transitioning from paper-based medication charts to electronic medication management (eMM) on DDIs and patient harms.</p><p><strong>Methods: </strong>This was a secondary analysis of the control arm of a controlled pre-post study. Patients were randomly selected from three Australian hospitals. Retrospective chart review was conducted before and after the implementation of an eMM system, without accompanying clinical decision support alerts for DDIs. Harm was assessed by an expert panel.</p><p><strong>Results: </strong>Of 1186 patient admissions, 70.1% (n = 831) experienced a pDDI, 42.6% (n = 505) a cDDI and 0.9% (n = 11) an actual harm in hospital. Of 15,860 pDDIs identified, 27.0% (n = 4285) were classified as cDDIs. The median number of pDDIs and cDDIs per 10 drugs were 6 [interquartile range (IQR) 2-13] and 0 (IQR 0-2), respectively. In cases where a cDDI was identified, both drugs were 44% less likely to be co-administered following eMM (adjusted odds ratio 0.56, 95% confidence interval 0.46-0.73).</p><p><strong>Conclusion: </strong>Although most patients experienced a pDDI during their hospital stay, less than one-third of pDDIs were clinically relevant. The low prevalence of harm identified raises questions about the value of incorporating DDI decision support into systems given the potential negative impacts of DDI alerts.</p>","PeriodicalId":11382,"journal":{"name":"Drug Safety","volume":" ","pages":"557-569"},"PeriodicalIF":3.8000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11116265/pdf/","citationCount":"0","resultStr":"{\"title\":\"Drug-Drug Interactions and Actual Harm to Hospitalized Patients: A Multicentre Study Examining the Prevalence Pre- and Post-Electronic Medication System Implementation.\",\"authors\":\"Ling Li, Jannah Baker, Renee Quirk, Danielle Deidun, Maria Moran, Ahmed Abo Salem, Nanda Aryal, Bethany A Van Dort, Wu Yi Zheng, Andrew Hargreaves, Paula Doherty, Sarah N Hilmer, Richard O Day, Johanna I Westbrook, Melissa T Baysari\",\"doi\":\"10.1007/s40264-024-01412-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Drug-drug interactions (DDIs) have potential to cause patient harm, including lowering therapeutic efficacy. This study aimed to (i) determine the prevalence of potential DDIs (pDDIs); clinically relevant DDIs (cDDIs), that is, DDIs that could lead to patient harm, taking into account a patient's individual clinical profile, drug effects and severity of potential harmful outcome; and subsequent actual harm among hospitalized patients and (ii) examine the impact of transitioning from paper-based medication charts to electronic medication management (eMM) on DDIs and patient harms.</p><p><strong>Methods: </strong>This was a secondary analysis of the control arm of a controlled pre-post study. Patients were randomly selected from three Australian hospitals. Retrospective chart review was conducted before and after the implementation of an eMM system, without accompanying clinical decision support alerts for DDIs. Harm was assessed by an expert panel.</p><p><strong>Results: </strong>Of 1186 patient admissions, 70.1% (n = 831) experienced a pDDI, 42.6% (n = 505) a cDDI and 0.9% (n = 11) an actual harm in hospital. Of 15,860 pDDIs identified, 27.0% (n = 4285) were classified as cDDIs. The median number of pDDIs and cDDIs per 10 drugs were 6 [interquartile range (IQR) 2-13] and 0 (IQR 0-2), respectively. In cases where a cDDI was identified, both drugs were 44% less likely to be co-administered following eMM (adjusted odds ratio 0.56, 95% confidence interval 0.46-0.73).</p><p><strong>Conclusion: </strong>Although most patients experienced a pDDI during their hospital stay, less than one-third of pDDIs were clinically relevant. The low prevalence of harm identified raises questions about the value of incorporating DDI decision support into systems given the potential negative impacts of DDI alerts.</p>\",\"PeriodicalId\":11382,\"journal\":{\"name\":\"Drug Safety\",\"volume\":\" \",\"pages\":\"557-569\"},\"PeriodicalIF\":3.8000,\"publicationDate\":\"2024-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11116265/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Drug Safety\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s40264-024-01412-w\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/3/13 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"PHARMACOLOGY & PHARMACY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drug Safety","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40264-024-01412-w","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/13 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
Drug-Drug Interactions and Actual Harm to Hospitalized Patients: A Multicentre Study Examining the Prevalence Pre- and Post-Electronic Medication System Implementation.
Introduction: Drug-drug interactions (DDIs) have potential to cause patient harm, including lowering therapeutic efficacy. This study aimed to (i) determine the prevalence of potential DDIs (pDDIs); clinically relevant DDIs (cDDIs), that is, DDIs that could lead to patient harm, taking into account a patient's individual clinical profile, drug effects and severity of potential harmful outcome; and subsequent actual harm among hospitalized patients and (ii) examine the impact of transitioning from paper-based medication charts to electronic medication management (eMM) on DDIs and patient harms.
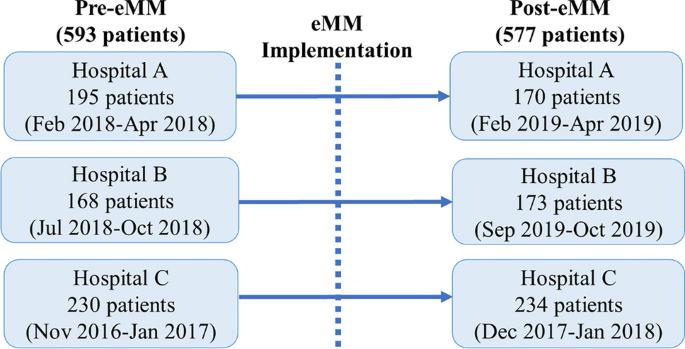
Methods: This was a secondary analysis of the control arm of a controlled pre-post study. Patients were randomly selected from three Australian hospitals. Retrospective chart review was conducted before and after the implementation of an eMM system, without accompanying clinical decision support alerts for DDIs. Harm was assessed by an expert panel.
Results: Of 1186 patient admissions, 70.1% (n = 831) experienced a pDDI, 42.6% (n = 505) a cDDI and 0.9% (n = 11) an actual harm in hospital. Of 15,860 pDDIs identified, 27.0% (n = 4285) were classified as cDDIs. The median number of pDDIs and cDDIs per 10 drugs were 6 [interquartile range (IQR) 2-13] and 0 (IQR 0-2), respectively. In cases where a cDDI was identified, both drugs were 44% less likely to be co-administered following eMM (adjusted odds ratio 0.56, 95% confidence interval 0.46-0.73).
Conclusion: Although most patients experienced a pDDI during their hospital stay, less than one-third of pDDIs were clinically relevant. The low prevalence of harm identified raises questions about the value of incorporating DDI decision support into systems given the potential negative impacts of DDI alerts.
期刊介绍:
Drug Safety is the official journal of the International Society of Pharmacovigilance. The journal includes:
Overviews of contentious or emerging issues.
Comprehensive narrative reviews that provide an authoritative source of information on epidemiology, clinical features, prevention and management of adverse effects of individual drugs and drug classes.
In-depth benefit-risk assessment of adverse effect and efficacy data for a drug in a defined therapeutic area.
Systematic reviews (with or without meta-analyses) that collate empirical evidence to answer a specific research question, using explicit, systematic methods as outlined by the PRISMA statement.
Original research articles reporting the results of well-designed studies in disciplines such as pharmacoepidemiology, pharmacovigilance, pharmacology and toxicology, and pharmacogenomics.
Editorials and commentaries on topical issues.
Additional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in Drug Safety Drugs may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand important medical advances.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
