Geok Hoon Lim, John Carson Allen, Yien Sien Lee, Sze Yiun Teo, Li Ching Lau, Thida Win, Lester Chee Hao Leong
{"title":"在基因组检测时代利用腋窝超声指导乳腺癌治疗。","authors":"Geok Hoon Lim, John Carson Allen, Yien Sien Lee, Sze Yiun Teo, Li Ching Lau, Thida Win, Lester Chee Hao Leong","doi":"10.3233/BD-230032","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Chemotherapy is conventionally offered to non-stage IV breast cancer patients with metastatic nodes. However, the RxPONDER trial showed that chemotherapy can be omitted in selected patients with 1-3 metastatic nodes if the 21-gene assay recurrence score is ≤25. We aimed to investigate if axillary ultrasound can identify this group of patients with limited nodal burden so that they can undergo upfront surgery followed by gene assay testing, to potentially avoid chemotherapy.</p><p><strong>Methods: </strong>T1-3, node positive, hormone receptor-positive and HER2-negative breast cancer patients ≥50 years old with axillary lymph node dissection (ALND) were reviewed from 2 centres. Patients with neoadjuvant chemotherapy and bilateral cancers were excluded. Number of ultrasound-detected abnormal axillary nodes, demographic and histological parameters were correlated with the number of metastatic nodes found on ALND.</p><p><strong>Results: </strong>138 patients were included, 59 (42.8%) and 79 (57.2%) patients had 1-3 and >3 metastatic nodes on ALND respectively. On logistic regression and ROC analysis, the number of ultrasound-detected abnormal nodes was significant (p < 0.001) for predicting limited nodal burden (ROC AUC = 0.7135). Probabilities of <4 metastatic nodes with ultrasound cut-offs of 5, 6 and 8 abnormal nodes were 0.057, 0.026 and 0.005 respectively, with 100% specificity.</p><p><strong>Conclusion: </strong>A cut-off of ≤5 ultrasound-detected abnormal nodes can distinguish between patients with limited versus high nodal burden, with high specificity. Hence, incorporating the number of abnormal ultrasound-detected nodes into clinical practice may prove useful in guiding between upfront surgery and gene assay testing or neoadjuvant chemotherapy in this group of patients.</p>","PeriodicalId":9224,"journal":{"name":"Breast disease","volume":"43 1","pages":"19-23"},"PeriodicalIF":0.0000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10977404/pdf/","citationCount":"0","resultStr":"{\"title\":\"Use of axillary ultrasound to guide breast cancer management in the genomic assay era.\",\"authors\":\"Geok Hoon Lim, John Carson Allen, Yien Sien Lee, Sze Yiun Teo, Li Ching Lau, Thida Win, Lester Chee Hao Leong\",\"doi\":\"10.3233/BD-230032\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Chemotherapy is conventionally offered to non-stage IV breast cancer patients with metastatic nodes. However, the RxPONDER trial showed that chemotherapy can be omitted in selected patients with 1-3 metastatic nodes if the 21-gene assay recurrence score is ≤25. We aimed to investigate if axillary ultrasound can identify this group of patients with limited nodal burden so that they can undergo upfront surgery followed by gene assay testing, to potentially avoid chemotherapy.</p><p><strong>Methods: </strong>T1-3, node positive, hormone receptor-positive and HER2-negative breast cancer patients ≥50 years old with axillary lymph node dissection (ALND) were reviewed from 2 centres. Patients with neoadjuvant chemotherapy and bilateral cancers were excluded. Number of ultrasound-detected abnormal axillary nodes, demographic and histological parameters were correlated with the number of metastatic nodes found on ALND.</p><p><strong>Results: </strong>138 patients were included, 59 (42.8%) and 79 (57.2%) patients had 1-3 and >3 metastatic nodes on ALND respectively. On logistic regression and ROC analysis, the number of ultrasound-detected abnormal nodes was significant (p < 0.001) for predicting limited nodal burden (ROC AUC = 0.7135). Probabilities of <4 metastatic nodes with ultrasound cut-offs of 5, 6 and 8 abnormal nodes were 0.057, 0.026 and 0.005 respectively, with 100% specificity.</p><p><strong>Conclusion: </strong>A cut-off of ≤5 ultrasound-detected abnormal nodes can distinguish between patients with limited versus high nodal burden, with high specificity. Hence, incorporating the number of abnormal ultrasound-detected nodes into clinical practice may prove useful in guiding between upfront surgery and gene assay testing or neoadjuvant chemotherapy in this group of patients.</p>\",\"PeriodicalId\":9224,\"journal\":{\"name\":\"Breast disease\",\"volume\":\"43 1\",\"pages\":\"19-23\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10977404/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Breast disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3233/BD-230032\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Breast disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3233/BD-230032","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Use of axillary ultrasound to guide breast cancer management in the genomic assay era.
Introduction: Chemotherapy is conventionally offered to non-stage IV breast cancer patients with metastatic nodes. However, the RxPONDER trial showed that chemotherapy can be omitted in selected patients with 1-3 metastatic nodes if the 21-gene assay recurrence score is ≤25. We aimed to investigate if axillary ultrasound can identify this group of patients with limited nodal burden so that they can undergo upfront surgery followed by gene assay testing, to potentially avoid chemotherapy.
Methods: T1-3, node positive, hormone receptor-positive and HER2-negative breast cancer patients ≥50 years old with axillary lymph node dissection (ALND) were reviewed from 2 centres. Patients with neoadjuvant chemotherapy and bilateral cancers were excluded. Number of ultrasound-detected abnormal axillary nodes, demographic and histological parameters were correlated with the number of metastatic nodes found on ALND.
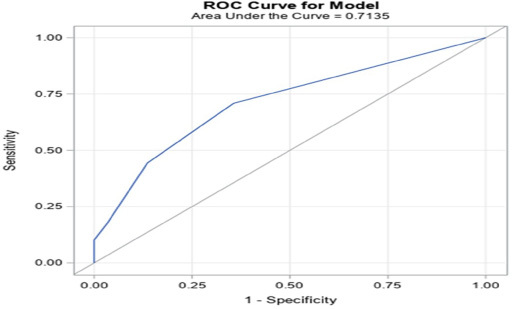
Results: 138 patients were included, 59 (42.8%) and 79 (57.2%) patients had 1-3 and >3 metastatic nodes on ALND respectively. On logistic regression and ROC analysis, the number of ultrasound-detected abnormal nodes was significant (p < 0.001) for predicting limited nodal burden (ROC AUC = 0.7135). Probabilities of <4 metastatic nodes with ultrasound cut-offs of 5, 6 and 8 abnormal nodes were 0.057, 0.026 and 0.005 respectively, with 100% specificity.
Conclusion: A cut-off of ≤5 ultrasound-detected abnormal nodes can distinguish between patients with limited versus high nodal burden, with high specificity. Hence, incorporating the number of abnormal ultrasound-detected nodes into clinical practice may prove useful in guiding between upfront surgery and gene assay testing or neoadjuvant chemotherapy in this group of patients.
期刊介绍:
The recent expansion of work in the field of breast cancer inevitably will hasten discoveries that will have impact on patient outcome. The breadth of this research that spans basic science, clinical medicine, epidemiology, and public policy poses difficulties for investigators. Not only is it necessary to be facile in comprehending ideas from many disciplines, but also important to understand the public implications of these discoveries. Breast Disease publishes review issues devoted to an in-depth analysis of the scientific and public implications of recent research on a specific problem in breast cancer. Thus, the reviews will not only discuss recent discoveries but will also reflect on their impact in breast cancer research or clinical management.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
