Aleksander Dokollari, Serge Sicouri, Leila Hosseinian, Ozgun Erten, Basel Ramlawi, Gianluigi Bisleri, Massimo Bonacchi, Noah Sicouri, Gianluca Torregrossa, Francis P Sutter
{"title":"影响冠状动脉旁路移植术慢性阻塞性肺病患者长期预后的围手术期风险预测因子","authors":"Aleksander Dokollari, Serge Sicouri, Leila Hosseinian, Ozgun Erten, Basel Ramlawi, Gianluigi Bisleri, Massimo Bonacchi, Noah Sicouri, Gianluca Torregrossa, Francis P Sutter","doi":"10.14503/THIJ-23-8199","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This study sought to identify periprocedural risk predictors that affect long-term prognosis in patients with chronic obstructive pulmonary disease (COPD) undergoing isolated coronary artery bypass grafting (CABG).</p><p><strong>Methods: </strong>All consecutive 4,871 patients undergoing isolated CABG between May 2005 and June 2021 were included. Patients with and without COPD were compared for baseline demographics and preoperative characteristics. A propensity-matched analysis was used to compare the 2 groups. The primary outcome was long-term incidence of all-cause death.</p><p><strong>Results: </strong>After matching, 767 patients each were included in the COPD and non-COPD groups; mean age was 71.6 and 71.4 years (P = .7), respectively; 29.3% and 32% (P = .2) were women, respectively. Intraoperatively, median (IQR) operating room time was higher in the COPD group than in the non-COPD group (5.9 [5.2-7.0] hours vs 5.8 [5.1-6.7] hours, respectively; P = .01). Postoperatively, intensive care unit stay (P = .03), hospital length of stay (P = .0004), and fresh frozen plasma transfusion units (P = .012) were higher in the COPD group than in the non-COPD group. Thirty-day mortality was not different between groups (1.3% in the COPD group vs 1% in the non-COPD group; P = .4). Median follow-up time was 4.0 years. The rate of all-cause death was higher in the COPD group than in the non-COPD group (138 patients [18.3%] vs 109 patients [14.5%], respectively; P = .042). Periprocedural risk predictors for all-cause death in patients with COPD were atrial fibrillation, diabetes, male sex, dialysis, ejection fraction less than 50%, peripheral vascular disease, and Society of Thoracic Surgeons Predicted Risk of Mortality score greater than 4%.</p><p><strong>Conclusion: </strong>Patients with COPD undergoing isolated CABG had a significantly higher incidence of all-cause death than those without COPD. Herein, risk predictors are provided for all-cause death in patients undergoing isolated CABG.</p>","PeriodicalId":48680,"journal":{"name":"Texas Heart Institute Journal","volume":"51 1","pages":""},"PeriodicalIF":0.9000,"publicationDate":"2024-03-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11075519/pdf/","citationCount":"0","resultStr":"{\"title\":\"Periprocedural Risk Predictors Affecting Long-Term Prognosis in Patients With Chronic Obstructive Pulmonary Disease Undergoing Coronary Artery Bypass Grafting.\",\"authors\":\"Aleksander Dokollari, Serge Sicouri, Leila Hosseinian, Ozgun Erten, Basel Ramlawi, Gianluigi Bisleri, Massimo Bonacchi, Noah Sicouri, Gianluca Torregrossa, Francis P Sutter\",\"doi\":\"10.14503/THIJ-23-8199\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>This study sought to identify periprocedural risk predictors that affect long-term prognosis in patients with chronic obstructive pulmonary disease (COPD) undergoing isolated coronary artery bypass grafting (CABG).</p><p><strong>Methods: </strong>All consecutive 4,871 patients undergoing isolated CABG between May 2005 and June 2021 were included. Patients with and without COPD were compared for baseline demographics and preoperative characteristics. A propensity-matched analysis was used to compare the 2 groups. The primary outcome was long-term incidence of all-cause death.</p><p><strong>Results: </strong>After matching, 767 patients each were included in the COPD and non-COPD groups; mean age was 71.6 and 71.4 years (P = .7), respectively; 29.3% and 32% (P = .2) were women, respectively. Intraoperatively, median (IQR) operating room time was higher in the COPD group than in the non-COPD group (5.9 [5.2-7.0] hours vs 5.8 [5.1-6.7] hours, respectively; P = .01). Postoperatively, intensive care unit stay (P = .03), hospital length of stay (P = .0004), and fresh frozen plasma transfusion units (P = .012) were higher in the COPD group than in the non-COPD group. Thirty-day mortality was not different between groups (1.3% in the COPD group vs 1% in the non-COPD group; P = .4). Median follow-up time was 4.0 years. The rate of all-cause death was higher in the COPD group than in the non-COPD group (138 patients [18.3%] vs 109 patients [14.5%], respectively; P = .042). Periprocedural risk predictors for all-cause death in patients with COPD were atrial fibrillation, diabetes, male sex, dialysis, ejection fraction less than 50%, peripheral vascular disease, and Society of Thoracic Surgeons Predicted Risk of Mortality score greater than 4%.</p><p><strong>Conclusion: </strong>Patients with COPD undergoing isolated CABG had a significantly higher incidence of all-cause death than those without COPD. Herein, risk predictors are provided for all-cause death in patients undergoing isolated CABG.</p>\",\"PeriodicalId\":48680,\"journal\":{\"name\":\"Texas Heart Institute Journal\",\"volume\":\"51 1\",\"pages\":\"\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2024-03-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11075519/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Texas Heart Institute Journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.14503/THIJ-23-8199\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Texas Heart Institute Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14503/THIJ-23-8199","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Periprocedural Risk Predictors Affecting Long-Term Prognosis in Patients With Chronic Obstructive Pulmonary Disease Undergoing Coronary Artery Bypass Grafting.
Objective: This study sought to identify periprocedural risk predictors that affect long-term prognosis in patients with chronic obstructive pulmonary disease (COPD) undergoing isolated coronary artery bypass grafting (CABG).
Methods: All consecutive 4,871 patients undergoing isolated CABG between May 2005 and June 2021 were included. Patients with and without COPD were compared for baseline demographics and preoperative characteristics. A propensity-matched analysis was used to compare the 2 groups. The primary outcome was long-term incidence of all-cause death.
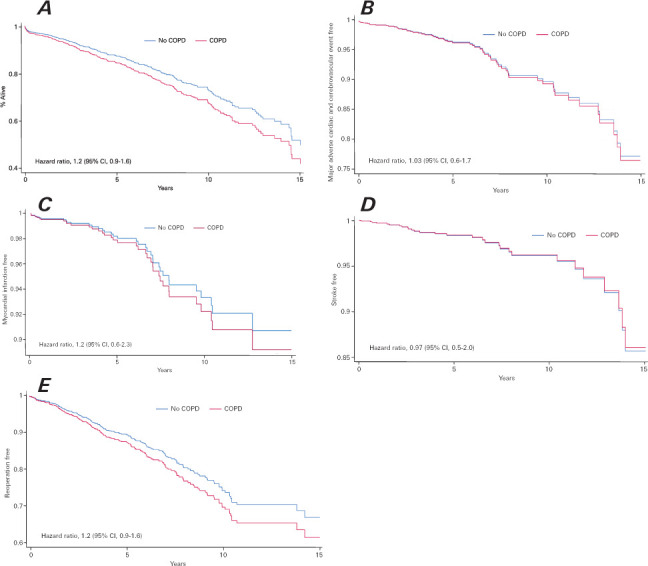
Results: After matching, 767 patients each were included in the COPD and non-COPD groups; mean age was 71.6 and 71.4 years (P = .7), respectively; 29.3% and 32% (P = .2) were women, respectively. Intraoperatively, median (IQR) operating room time was higher in the COPD group than in the non-COPD group (5.9 [5.2-7.0] hours vs 5.8 [5.1-6.7] hours, respectively; P = .01). Postoperatively, intensive care unit stay (P = .03), hospital length of stay (P = .0004), and fresh frozen plasma transfusion units (P = .012) were higher in the COPD group than in the non-COPD group. Thirty-day mortality was not different between groups (1.3% in the COPD group vs 1% in the non-COPD group; P = .4). Median follow-up time was 4.0 years. The rate of all-cause death was higher in the COPD group than in the non-COPD group (138 patients [18.3%] vs 109 patients [14.5%], respectively; P = .042). Periprocedural risk predictors for all-cause death in patients with COPD were atrial fibrillation, diabetes, male sex, dialysis, ejection fraction less than 50%, peripheral vascular disease, and Society of Thoracic Surgeons Predicted Risk of Mortality score greater than 4%.
Conclusion: Patients with COPD undergoing isolated CABG had a significantly higher incidence of all-cause death than those without COPD. Herein, risk predictors are provided for all-cause death in patients undergoing isolated CABG.
期刊介绍:
For more than 45 years, the Texas Heart Institute Journal has been published by the Texas Heart Institute as part of its medical education program. Our bimonthly peer-reviewed journal enjoys a global audience of physicians, scientists, and healthcare professionals who are contributing to the prevention, diagnosis, and treatment of cardiovascular disease.
The Journal was printed under the name of Cardiovascular Diseases from 1974 through 1981 (ISSN 0093-3546). The name was changed to Texas Heart Institute Journal in 1982 and was printed through 2013 (ISSN 0730-2347). In 2014, the Journal moved to online-only publication. It is indexed by Index Medicus/MEDLINE and by other indexing and abstracting services worldwide. Our full archive is available at PubMed Central.
The Journal invites authors to submit these article types for review:
-Clinical Investigations-
Laboratory Investigations-
Reviews-
Techniques-
Coronary Anomalies-
History of Medicine-
Case Reports/Case Series (Submission Fee: $70.00 USD)-
Images in Cardiovascular Medicine (Submission Fee: $35.00 USD)-
Guest Editorials-
Peabody’s Corner-
Letters to the Editor




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
