Rachel Goldstein, Natalie Rabkin, Noa Buchman, Aviya R Jacobs, Khaled Sandouka, Bruria Raccah, Tamar Fisher Negev, Ilan Matok, Meir Bialer, Mordechai Muszkat
{"title":"与酶诱导型抗癫痫药物相比,左乙拉西坦对阿哌沙班和利伐沙班血浆峰浓度的影响","authors":"Rachel Goldstein, Natalie Rabkin, Noa Buchman, Aviya R Jacobs, Khaled Sandouka, Bruria Raccah, Tamar Fisher Negev, Ilan Matok, Meir Bialer, Mordechai Muszkat","doi":"10.1007/s40263-024-01077-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objective: </strong>Post-stroke epilepsy represents an important clinical challenge as it often requires both treatment with direct oral anticoagulants (DOACs) and antiseizure medications (ASMs). Levetiracetam (LEV), an ASM not known to induce metabolizing enzymes, has been suggested as a safer alternative to enzyme-inducing (EI)-ASMs in patients treated with DOACs; however, current clinical guidelines suggest caution when LEV is used with DOACs because of possible P-glycoprotein induction and competition (based on preclinical studies). We investigated whether LEV affects apixaban and rivaroxaban concentrations compared with two control groups: (a) patients treated with EI-ASMs and (b) patients not treated with any ASM.</p><p><strong>Methods: </strong>In this retrospective observational study, we monitored apixaban and rivaroxaban peak plasma concentrations (C<sub>max</sub>) in 203 patients treated with LEV (n = 28) and with EI-ASM (n = 33), and in patients not treated with any ASM (n = 142). Enzyme-inducing ASMs included carbamazepine, phenytoin, phenobarbital, primidone, and oxcarbazepine. We collected clinical and laboratory data for analysis, and DOAC C<sub>max</sub> of patients taking LEV were compared with the other two groups.</p><p><strong>Results: </strong>In 203 patients, 55% were female and the mean age was 78 ± 0.8 years. One hundred and eighty-six patients received apixaban and 17 patients received rivaroxaban. The proportion of patients with DOAC C<sub>max</sub> below their therapeutic range was 7.1% in the LEV group, 10.6% in the non-ASM group, and 36.4% in the EI-ASM group (p < 0.001). The odds of having DOAC C<sub>max</sub> below the therapeutic range (compared with control groups) was not significantly different in patients taking LEV (adjusted odds ratio 0.70, 95% confidence interval 0.19-2.67, p = 0.61), but it was 12.7-fold higher in patients taking EI-ASM (p < 0.001). In an analysis in patients treated with apixaban, there was no difference in apixaban C<sub>max</sub> between patients treated with LEV and non-ASM controls, and LEV clinical use was not associated with variability in apixaban C<sub>max</sub> in a multivariate linear regression.</p><p><strong>Conclusions: </strong>In this study, we show that unlike EI-ASMs, LEV clinical use was not significantly associated with lower apixaban C<sub>max</sub> and was similar to that in patients not treated with any ASM. Our findings suggest that the combination of LEV with apixaban and rivaroxaban may not be associated with decreased apixaban and rivaroxaban C<sub>max</sub>. Therefore, prospective controlled studies are required to examine the possible non-pharmacokinetic mechanism of the effect of the LEV-apixaban or LEV-rivaroxaban combination on patients' outcomes.</p>","PeriodicalId":10508,"journal":{"name":"CNS drugs","volume":" ","pages":"399-408"},"PeriodicalIF":7.4000,"publicationDate":"2024-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11026229/pdf/","citationCount":"0","resultStr":"{\"title\":\"The Effect of Levetiracetam Compared with Enzyme-Inducing Antiseizure Medications on Apixaban and Rivaroxaban Peak Plasma Concentrations.\",\"authors\":\"Rachel Goldstein, Natalie Rabkin, Noa Buchman, Aviya R Jacobs, Khaled Sandouka, Bruria Raccah, Tamar Fisher Negev, Ilan Matok, Meir Bialer, Mordechai Muszkat\",\"doi\":\"10.1007/s40263-024-01077-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background and objective: </strong>Post-stroke epilepsy represents an important clinical challenge as it often requires both treatment with direct oral anticoagulants (DOACs) and antiseizure medications (ASMs). Levetiracetam (LEV), an ASM not known to induce metabolizing enzymes, has been suggested as a safer alternative to enzyme-inducing (EI)-ASMs in patients treated with DOACs; however, current clinical guidelines suggest caution when LEV is used with DOACs because of possible P-glycoprotein induction and competition (based on preclinical studies). We investigated whether LEV affects apixaban and rivaroxaban concentrations compared with two control groups: (a) patients treated with EI-ASMs and (b) patients not treated with any ASM.</p><p><strong>Methods: </strong>In this retrospective observational study, we monitored apixaban and rivaroxaban peak plasma concentrations (C<sub>max</sub>) in 203 patients treated with LEV (n = 28) and with EI-ASM (n = 33), and in patients not treated with any ASM (n = 142). Enzyme-inducing ASMs included carbamazepine, phenytoin, phenobarbital, primidone, and oxcarbazepine. We collected clinical and laboratory data for analysis, and DOAC C<sub>max</sub> of patients taking LEV were compared with the other two groups.</p><p><strong>Results: </strong>In 203 patients, 55% were female and the mean age was 78 ± 0.8 years. One hundred and eighty-six patients received apixaban and 17 patients received rivaroxaban. The proportion of patients with DOAC C<sub>max</sub> below their therapeutic range was 7.1% in the LEV group, 10.6% in the non-ASM group, and 36.4% in the EI-ASM group (p < 0.001). The odds of having DOAC C<sub>max</sub> below the therapeutic range (compared with control groups) was not significantly different in patients taking LEV (adjusted odds ratio 0.70, 95% confidence interval 0.19-2.67, p = 0.61), but it was 12.7-fold higher in patients taking EI-ASM (p < 0.001). In an analysis in patients treated with apixaban, there was no difference in apixaban C<sub>max</sub> between patients treated with LEV and non-ASM controls, and LEV clinical use was not associated with variability in apixaban C<sub>max</sub> in a multivariate linear regression.</p><p><strong>Conclusions: </strong>In this study, we show that unlike EI-ASMs, LEV clinical use was not significantly associated with lower apixaban C<sub>max</sub> and was similar to that in patients not treated with any ASM. Our findings suggest that the combination of LEV with apixaban and rivaroxaban may not be associated with decreased apixaban and rivaroxaban C<sub>max</sub>. Therefore, prospective controlled studies are required to examine the possible non-pharmacokinetic mechanism of the effect of the LEV-apixaban or LEV-rivaroxaban combination on patients' outcomes.</p>\",\"PeriodicalId\":10508,\"journal\":{\"name\":\"CNS drugs\",\"volume\":\" \",\"pages\":\"399-408\"},\"PeriodicalIF\":7.4000,\"publicationDate\":\"2024-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11026229/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"CNS drugs\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s40263-024-01077-0\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/3/23 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"CNS drugs","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40263-024-01077-0","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/23 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
The Effect of Levetiracetam Compared with Enzyme-Inducing Antiseizure Medications on Apixaban and Rivaroxaban Peak Plasma Concentrations.
Background and objective: Post-stroke epilepsy represents an important clinical challenge as it often requires both treatment with direct oral anticoagulants (DOACs) and antiseizure medications (ASMs). Levetiracetam (LEV), an ASM not known to induce metabolizing enzymes, has been suggested as a safer alternative to enzyme-inducing (EI)-ASMs in patients treated with DOACs; however, current clinical guidelines suggest caution when LEV is used with DOACs because of possible P-glycoprotein induction and competition (based on preclinical studies). We investigated whether LEV affects apixaban and rivaroxaban concentrations compared with two control groups: (a) patients treated with EI-ASMs and (b) patients not treated with any ASM.
Methods: In this retrospective observational study, we monitored apixaban and rivaroxaban peak plasma concentrations (Cmax) in 203 patients treated with LEV (n = 28) and with EI-ASM (n = 33), and in patients not treated with any ASM (n = 142). Enzyme-inducing ASMs included carbamazepine, phenytoin, phenobarbital, primidone, and oxcarbazepine. We collected clinical and laboratory data for analysis, and DOAC Cmax of patients taking LEV were compared with the other two groups.
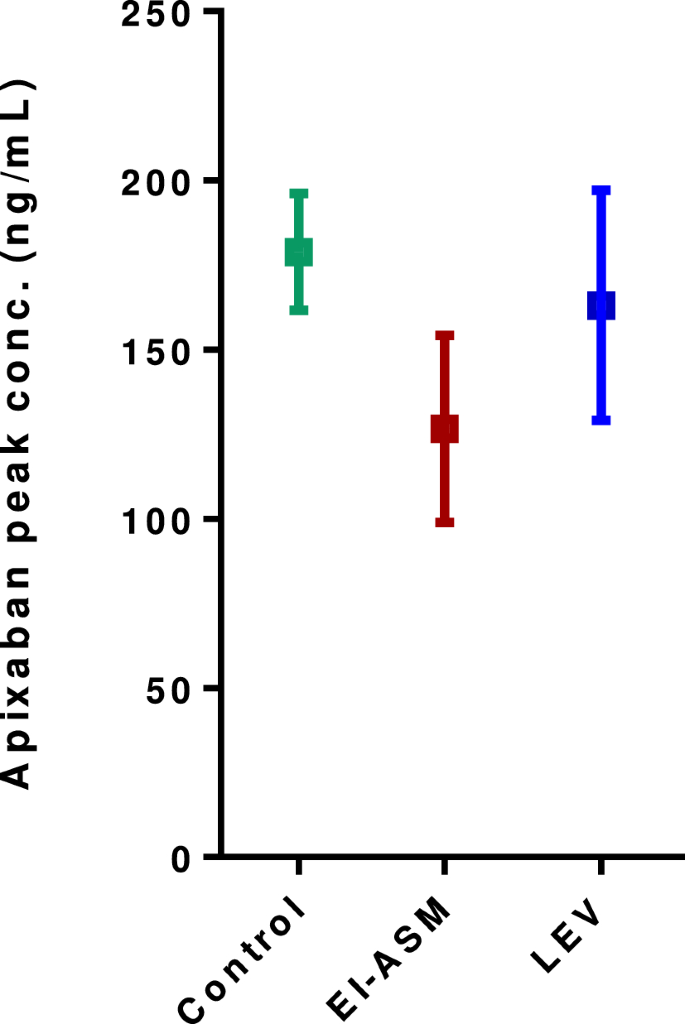
Results: In 203 patients, 55% were female and the mean age was 78 ± 0.8 years. One hundred and eighty-six patients received apixaban and 17 patients received rivaroxaban. The proportion of patients with DOAC Cmax below their therapeutic range was 7.1% in the LEV group, 10.6% in the non-ASM group, and 36.4% in the EI-ASM group (p < 0.001). The odds of having DOAC Cmax below the therapeutic range (compared with control groups) was not significantly different in patients taking LEV (adjusted odds ratio 0.70, 95% confidence interval 0.19-2.67, p = 0.61), but it was 12.7-fold higher in patients taking EI-ASM (p < 0.001). In an analysis in patients treated with apixaban, there was no difference in apixaban Cmax between patients treated with LEV and non-ASM controls, and LEV clinical use was not associated with variability in apixaban Cmax in a multivariate linear regression.
Conclusions: In this study, we show that unlike EI-ASMs, LEV clinical use was not significantly associated with lower apixaban Cmax and was similar to that in patients not treated with any ASM. Our findings suggest that the combination of LEV with apixaban and rivaroxaban may not be associated with decreased apixaban and rivaroxaban Cmax. Therefore, prospective controlled studies are required to examine the possible non-pharmacokinetic mechanism of the effect of the LEV-apixaban or LEV-rivaroxaban combination on patients' outcomes.
期刊介绍:
CNS Drugs promotes rational pharmacotherapy within the disciplines of clinical psychiatry and neurology. The Journal includes:
- Overviews of contentious or emerging issues.
- Comprehensive narrative reviews that provide an authoritative source of information on pharmacological approaches to managing neurological and psychiatric illnesses.
- Systematic reviews that collate empirical evidence to answer a specific research question, using explicit, systematic methods as outlined by the PRISMA statement.
- Adis Drug Reviews of the properties and place in therapy of both newer and established drugs in neurology and psychiatry.
- Original research articles reporting the results of well-designed studies with a strong link to clinical practice, such as clinical pharmacodynamic and pharmacokinetic studies, clinical trials, meta-analyses, outcomes research, and pharmacoeconomic and pharmacoepidemiological studies.
Additional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in CNS Drugs may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand important medical advances.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
