Mohammad Alhasoon, Bader Alqahtani, Mohamad Alreefi, Abdulaziz Homedi, Ghadah Alnami, Saif Alsaif, Kamal Ali
{"title":"早产儿单胎和多胎新生儿死亡率和发病率的回顾性比较分析--单个中心的经验。","authors":"Mohammad Alhasoon, Bader Alqahtani, Mohamad Alreefi, Abdulaziz Homedi, Ghadah Alnami, Saif Alsaif, Kamal Ali","doi":"10.1177/2333794X241240571","DOIUrl":null,"url":null,"abstract":"<p><p><i>Objective.</i> To compare mortality and major neonatal morbidities between singleton preterm infants and preterm infants of multiple gestations born <33 weeks' gestation. <i>Method.</i> Case-control study of preterm multiples and singletons <33 weeks' born at King Abdul-Aziz Medical City Riyadh (KAMC-R) between January 2017 and December 2020. Out-born infants and infants with lethal congenital abnormalities were excluded from the study. Mortality and major neonatal morbidities including bronchopulmonary dysplasia (BPD), retinopathy of prematurity (ROP), sepsis and surgical necrotizing enterocolitis (NEC) were compared between preterm singletons and multiples. <i>Results.</i> A total of 803 preterm infants were included: 567 (70.6%) were singletons, 158 (19.6%) were twins and 36 (4.5%) infants were higher multiples. Adjusted mortality before hospital discharge was significantly higher among preterm infants of multiple gestations compared to preterm singletons (12.3% vs 7.9%; <i>P</i> = .003; AOR, 2.2; 95% CI, 1.3-3.7). Retinopathy of prematurity (ROP) needing treatment was significantly higher among preterm infants of multiple pregnancies compared to preterm singletons (11% vs 6.5%, <i>P</i> = .033, AOR 1.1, 95% CI, 1.04-2.99). In addition, the incidence of bronchopulmonary dysplasia (BPD) at 36 weeks post menstrual age (PMA) (29.7% vs 20.5%; P = .003; AOR, 1.7; 95% CI, 1.2-2.5) and culture positive sepsis (24.2% vs 17.5%; <i>P</i> = .044; AOR, 1.5; 95% CI, 1.01-2.2) were significantly higher among preterm infants of multiple pregnancy. There were no differences in mortality and adverse neonatal outcomes between twins and higher multiples. <i>Conclusion.</i> Preterm infants of multiple gestations suffered higher mortality and neonatal morbidities compared to preterm singleton infants despite a higher utilization of maternal antenatal steroids and better antenatal care.</p>","PeriodicalId":12576,"journal":{"name":"Global Pediatric Health","volume":"11 ","pages":"2333794X241240571"},"PeriodicalIF":1.4000,"publicationDate":"2024-03-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10964436/pdf/","citationCount":"0","resultStr":"{\"title\":\"Retrospective Comparative Analysis of Neonatal Mortality and Morbidity in Preterm Singleton and Multiple Births -Single Center Experience.\",\"authors\":\"Mohammad Alhasoon, Bader Alqahtani, Mohamad Alreefi, Abdulaziz Homedi, Ghadah Alnami, Saif Alsaif, Kamal Ali\",\"doi\":\"10.1177/2333794X241240571\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><i>Objective.</i> To compare mortality and major neonatal morbidities between singleton preterm infants and preterm infants of multiple gestations born <33 weeks' gestation. <i>Method.</i> Case-control study of preterm multiples and singletons <33 weeks' born at King Abdul-Aziz Medical City Riyadh (KAMC-R) between January 2017 and December 2020. Out-born infants and infants with lethal congenital abnormalities were excluded from the study. Mortality and major neonatal morbidities including bronchopulmonary dysplasia (BPD), retinopathy of prematurity (ROP), sepsis and surgical necrotizing enterocolitis (NEC) were compared between preterm singletons and multiples. <i>Results.</i> A total of 803 preterm infants were included: 567 (70.6%) were singletons, 158 (19.6%) were twins and 36 (4.5%) infants were higher multiples. Adjusted mortality before hospital discharge was significantly higher among preterm infants of multiple gestations compared to preterm singletons (12.3% vs 7.9%; <i>P</i> = .003; AOR, 2.2; 95% CI, 1.3-3.7). Retinopathy of prematurity (ROP) needing treatment was significantly higher among preterm infants of multiple pregnancies compared to preterm singletons (11% vs 6.5%, <i>P</i> = .033, AOR 1.1, 95% CI, 1.04-2.99). In addition, the incidence of bronchopulmonary dysplasia (BPD) at 36 weeks post menstrual age (PMA) (29.7% vs 20.5%; P = .003; AOR, 1.7; 95% CI, 1.2-2.5) and culture positive sepsis (24.2% vs 17.5%; <i>P</i> = .044; AOR, 1.5; 95% CI, 1.01-2.2) were significantly higher among preterm infants of multiple pregnancy. There were no differences in mortality and adverse neonatal outcomes between twins and higher multiples. <i>Conclusion.</i> Preterm infants of multiple gestations suffered higher mortality and neonatal morbidities compared to preterm singleton infants despite a higher utilization of maternal antenatal steroids and better antenatal care.</p>\",\"PeriodicalId\":12576,\"journal\":{\"name\":\"Global Pediatric Health\",\"volume\":\"11 \",\"pages\":\"2333794X241240571\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2024-03-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10964436/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Global Pediatric Health\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/2333794X241240571\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global Pediatric Health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/2333794X241240571","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
摘要
目的:比较单胎早产儿和多胎早产儿的死亡率和新生儿主要发病率。比较单胎早产儿和多胎早产儿的死亡率和新生儿主要发病情况 方法:病例对照研究对多胎早产儿和单胎早产儿进行病例对照研究 结果。共纳入 803 名早产儿:其中 567 例(70.6%)为单胎,158 例(19.6%)为双胞胎,36 例(4.5%)为多胎。与单胎早产儿相比,多胎早产儿出院前的调整死亡率明显更高(12.3% vs 7.9%;P = .003;AOR,2.2;95% CI,1.3-3.7)。与单胎早产儿相比,多胎早产儿中需要治疗的早产儿视网膜病变(ROP)明显更高(11% vs 6.5%,P = .033,AOR 1.1,95% CI,1.04-2.99)。此外,多胎妊娠早产儿在月经后 36 周(PMA)支气管肺发育不良(BPD)(29.7% vs 20.5%;P = .003;AOR,1.7;95% CI,1.2-2.5)和败血症培养阳性(24.2% vs 17.5%;P = .044;AOR,1.5;95% CI,1.01-2.2)的发生率也明显高于单胎早产儿(11% vs 6.5%;P = .033;AOR,1.1;95% CI,1.04-2.99)。双胞胎和高龄多胞胎的死亡率和新生儿不良结局没有差异。结论与单胎早产儿相比,多胎早产儿的死亡率和新生儿发病率更高,尽管产妇产前使用类固醇的比例更高,产前护理也更好。
Retrospective Comparative Analysis of Neonatal Mortality and Morbidity in Preterm Singleton and Multiple Births -Single Center Experience.
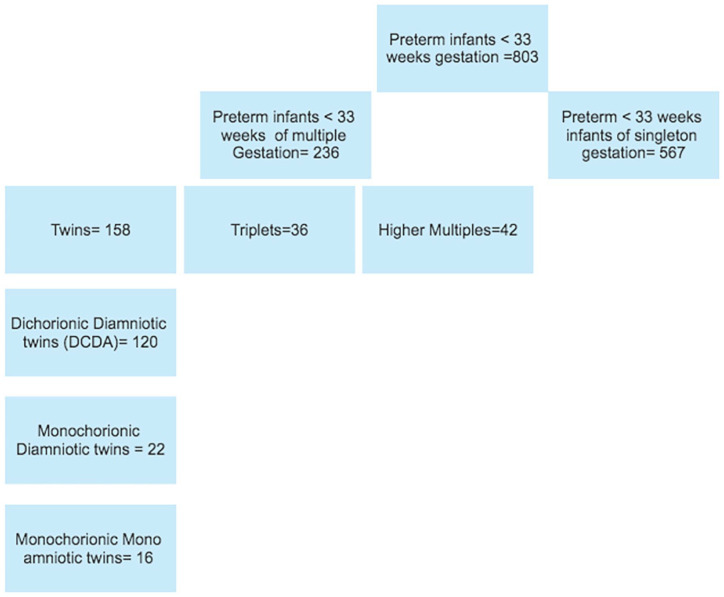
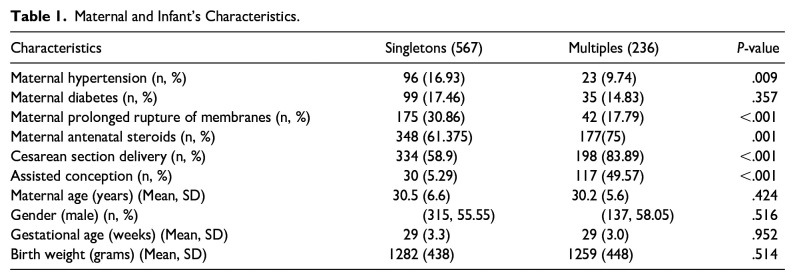
Objective. To compare mortality and major neonatal morbidities between singleton preterm infants and preterm infants of multiple gestations born <33 weeks' gestation. Method. Case-control study of preterm multiples and singletons <33 weeks' born at King Abdul-Aziz Medical City Riyadh (KAMC-R) between January 2017 and December 2020. Out-born infants and infants with lethal congenital abnormalities were excluded from the study. Mortality and major neonatal morbidities including bronchopulmonary dysplasia (BPD), retinopathy of prematurity (ROP), sepsis and surgical necrotizing enterocolitis (NEC) were compared between preterm singletons and multiples. Results. A total of 803 preterm infants were included: 567 (70.6%) were singletons, 158 (19.6%) were twins and 36 (4.5%) infants were higher multiples. Adjusted mortality before hospital discharge was significantly higher among preterm infants of multiple gestations compared to preterm singletons (12.3% vs 7.9%; P = .003; AOR, 2.2; 95% CI, 1.3-3.7). Retinopathy of prematurity (ROP) needing treatment was significantly higher among preterm infants of multiple pregnancies compared to preterm singletons (11% vs 6.5%, P = .033, AOR 1.1, 95% CI, 1.04-2.99). In addition, the incidence of bronchopulmonary dysplasia (BPD) at 36 weeks post menstrual age (PMA) (29.7% vs 20.5%; P = .003; AOR, 1.7; 95% CI, 1.2-2.5) and culture positive sepsis (24.2% vs 17.5%; P = .044; AOR, 1.5; 95% CI, 1.01-2.2) were significantly higher among preterm infants of multiple pregnancy. There were no differences in mortality and adverse neonatal outcomes between twins and higher multiples. Conclusion. Preterm infants of multiple gestations suffered higher mortality and neonatal morbidities compared to preterm singleton infants despite a higher utilization of maternal antenatal steroids and better antenatal care.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
