Ying Liu MM, Wen Li MM, Shuoyan An MD, Zhengqin Zhai MD, Xinju Liu RN, Mengxue Hei MBBS, Gailing Chen MD, PhD
{"title":"急性心肌梗死患者 24 小时血压变化与死亡率之间的关系。","authors":"Ying Liu MM, Wen Li MM, Shuoyan An MD, Zhengqin Zhai MD, Xinju Liu RN, Mengxue Hei MBBS, Gailing Chen MD, PhD","doi":"10.1002/clc.24261","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>In recent years, the mortality of patients with AMI has not declined significantly. The relationship between blood pressure variability (BPV) and acute myocardial infarction (AMI) is unclear. We explored the relationship between 24-h BPV and mortality in patients with AMI.</p>\n </section>\n \n <section>\n \n <h3> Hypothesis</h3>\n \n <p>The mortality of patients with AMI is related to BPV. We hope to provide therapeutic ideas for reducing the risk of death in patients with AMI.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This is a retrospective cohort study. We extracted and analyzed data from the MIMIC-IV 2.0, which was established in 1999 under the auspices of the National Institutes of Health (America). The average real variability (ARV) was calculated for the first 24-h blood pressure measurement after patients with AMI were admitted to the intensive care unit (ICU). Patients were divided into four groups according to ARV quartiles. The outcomes were 30-day, 1-year, and 3-year all-cause mortalities. Data were analyzed using Cox regression, Kaplan–Meier curves, and restricted cubic spline (RCS) curves.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>We enrolled 1291 patients with AMI, including 475 female. The patients were divided into four groups according to the qualities of diastolic blood pressure (DBP)-ARV. There were significant differences in the 30-day, 1-year and 3-year mortality among the four groups (<i>p</i> = .02, <i>p</i> < .001, <i>p</i> < .001, respectively). After adjustment for confounding factors, systolic blood pressure (SBP)-ARV could not predict AMI patient mortality (<i>p</i> > .05), while the highest DBP-ARV was associated strongly with increased 30-day mortality (HR: 2.291, 95% CI 1.260-4.168), 1-year mortality (HR: 1.933, 95% CI 1.316-2.840) and 3-year mortality (HR: 1.743, 95% CI 1.235-2.461). Kaplan–Meier curves demonstrated that, regardless of SBP or DBP, the long-term survival probabilities of patients in the highest ARV group were significantly lower than that of those in other groups. RCS curves showed that the death risk of patients with AMI first decreased and then increased with the increase in ARV when DBP-ARV < 8.04. The 30-day death risk first increased and then decreased, and the 1-year and 3-year death risks increased and then stabilized with ARV increase when DBP-ARV > 8.04.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>This study showed that patients with AMI may have an increased risk of short- and long-term death if their DBP-ARV is higher or lower during the first 24-h in ICU.</p>\n </section>\n </div>","PeriodicalId":10201,"journal":{"name":"Clinical Cardiology","volume":"47 4","pages":""},"PeriodicalIF":2.3000,"publicationDate":"2024-04-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clc.24261","citationCount":"0","resultStr":"{\"title\":\"Relationship between 24 h blood pressure variability and mortality in acute myocardial infarction patients\",\"authors\":\"Ying Liu MM, Wen Li MM, Shuoyan An MD, Zhengqin Zhai MD, Xinju Liu RN, Mengxue Hei MBBS, Gailing Chen MD, PhD\",\"doi\":\"10.1002/clc.24261\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>In recent years, the mortality of patients with AMI has not declined significantly. The relationship between blood pressure variability (BPV) and acute myocardial infarction (AMI) is unclear. We explored the relationship between 24-h BPV and mortality in patients with AMI.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Hypothesis</h3>\\n \\n <p>The mortality of patients with AMI is related to BPV. We hope to provide therapeutic ideas for reducing the risk of death in patients with AMI.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>This is a retrospective cohort study. We extracted and analyzed data from the MIMIC-IV 2.0, which was established in 1999 under the auspices of the National Institutes of Health (America). The average real variability (ARV) was calculated for the first 24-h blood pressure measurement after patients with AMI were admitted to the intensive care unit (ICU). Patients were divided into four groups according to ARV quartiles. The outcomes were 30-day, 1-year, and 3-year all-cause mortalities. Data were analyzed using Cox regression, Kaplan–Meier curves, and restricted cubic spline (RCS) curves.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>We enrolled 1291 patients with AMI, including 475 female. The patients were divided into four groups according to the qualities of diastolic blood pressure (DBP)-ARV. There were significant differences in the 30-day, 1-year and 3-year mortality among the four groups (<i>p</i> = .02, <i>p</i> < .001, <i>p</i> < .001, respectively). After adjustment for confounding factors, systolic blood pressure (SBP)-ARV could not predict AMI patient mortality (<i>p</i> > .05), while the highest DBP-ARV was associated strongly with increased 30-day mortality (HR: 2.291, 95% CI 1.260-4.168), 1-year mortality (HR: 1.933, 95% CI 1.316-2.840) and 3-year mortality (HR: 1.743, 95% CI 1.235-2.461). Kaplan–Meier curves demonstrated that, regardless of SBP or DBP, the long-term survival probabilities of patients in the highest ARV group were significantly lower than that of those in other groups. RCS curves showed that the death risk of patients with AMI first decreased and then increased with the increase in ARV when DBP-ARV < 8.04. The 30-day death risk first increased and then decreased, and the 1-year and 3-year death risks increased and then stabilized with ARV increase when DBP-ARV > 8.04.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>This study showed that patients with AMI may have an increased risk of short- and long-term death if their DBP-ARV is higher or lower during the first 24-h in ICU.</p>\\n </section>\\n </div>\",\"PeriodicalId\":10201,\"journal\":{\"name\":\"Clinical Cardiology\",\"volume\":\"47 4\",\"pages\":\"\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2024-04-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/clc.24261\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Cardiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/clc.24261\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Cardiology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/clc.24261","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:近年来,急性心肌梗死患者的死亡率并未明显下降。血压变异性(BPV)与急性心肌梗死(AMI)之间的关系尚不清楚。我们探讨了 24 小时血压变异与急性心肌梗死患者死亡率之间的关系:假设:急性心肌梗死患者的死亡率与血压波动有关。我们希望为降低 AMI 患者的死亡风险提供治疗思路:这是一项回顾性队列研究。我们从 MIMIC-IV 2.0 中提取并分析了数据,MIMIC-IV 2.0 于 1999 年在美国国立卫生研究院(National Institutes of Health)的支持下建立。我们计算了急性心肌梗死患者入住重症监护室(ICU)后首次 24 小时血压测量的平均实际变异率(ARV)。根据 ARV 四分位数将患者分为四组。结果为 30 天、1 年和 3 年全因死亡率。数据采用 Cox 回归、Kaplan-Meier 曲线和限制性立方样条曲线(RCS)进行分析:我们共收治了 1291 名 AMI 患者,其中包括 475 名女性。根据舒张压(DBP)-ARV 的质量将患者分为四组。四组患者的 30 天、1 年和 3 年死亡率存在明显差异(P = .02,P .05),而最高 DBP-ARV 与 30 天死亡率(HR:2.291,95% CI 1.260-4.168)、1 年死亡率(HR:1.933,95% CI 1.316-2.840)和 3 年死亡率(HR:1.743,95% CI 1.235-2.461)的增加密切相关。Kaplan-Meier 曲线显示,无论 SBP 或 DBP 如何,抗逆转录病毒药物剂量最高组患者的长期生存概率均显著低于其他组别。RCS曲线显示,当DBP-ARV为8.04时,随着ARV的增加,AMI患者的死亡风险先下降后上升:本研究表明,如果急性心肌梗死患者在入住重症监护室的前 24 小时内 DBP-ARV 升高或降低,其短期和长期死亡风险都会增加。
Relationship between 24 h blood pressure variability and mortality in acute myocardial infarction patients
Background
In recent years, the mortality of patients with AMI has not declined significantly. The relationship between blood pressure variability (BPV) and acute myocardial infarction (AMI) is unclear. We explored the relationship between 24-h BPV and mortality in patients with AMI.
Hypothesis
The mortality of patients with AMI is related to BPV. We hope to provide therapeutic ideas for reducing the risk of death in patients with AMI.
Methods
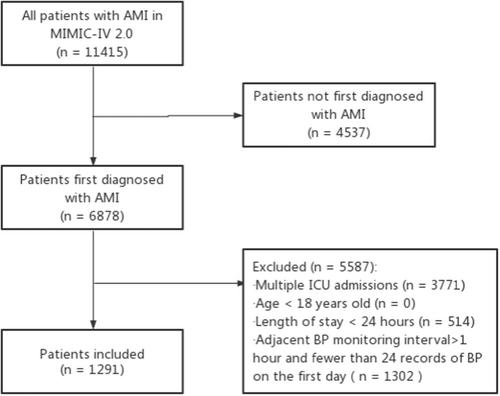
This is a retrospective cohort study. We extracted and analyzed data from the MIMIC-IV 2.0, which was established in 1999 under the auspices of the National Institutes of Health (America). The average real variability (ARV) was calculated for the first 24-h blood pressure measurement after patients with AMI were admitted to the intensive care unit (ICU). Patients were divided into four groups according to ARV quartiles. The outcomes were 30-day, 1-year, and 3-year all-cause mortalities. Data were analyzed using Cox regression, Kaplan–Meier curves, and restricted cubic spline (RCS) curves.
Results
We enrolled 1291 patients with AMI, including 475 female. The patients were divided into four groups according to the qualities of diastolic blood pressure (DBP)-ARV. There were significant differences in the 30-day, 1-year and 3-year mortality among the four groups (p = .02, p < .001, p < .001, respectively). After adjustment for confounding factors, systolic blood pressure (SBP)-ARV could not predict AMI patient mortality (p > .05), while the highest DBP-ARV was associated strongly with increased 30-day mortality (HR: 2.291, 95% CI 1.260-4.168), 1-year mortality (HR: 1.933, 95% CI 1.316-2.840) and 3-year mortality (HR: 1.743, 95% CI 1.235-2.461). Kaplan–Meier curves demonstrated that, regardless of SBP or DBP, the long-term survival probabilities of patients in the highest ARV group were significantly lower than that of those in other groups. RCS curves showed that the death risk of patients with AMI first decreased and then increased with the increase in ARV when DBP-ARV < 8.04. The 30-day death risk first increased and then decreased, and the 1-year and 3-year death risks increased and then stabilized with ARV increase when DBP-ARV > 8.04.
Conclusion
This study showed that patients with AMI may have an increased risk of short- and long-term death if their DBP-ARV is higher or lower during the first 24-h in ICU.
期刊介绍:
Clinical Cardiology provides a fully Gold Open Access forum for the publication of original clinical research, as well as brief reviews of diagnostic and therapeutic issues in cardiovascular medicine and cardiovascular surgery.
The journal includes Clinical Investigations, Reviews, free standing editorials and commentaries, and bonus online-only content.
The journal also publishes supplements, Expert Panel Discussions, sponsored clinical Reviews, Trial Designs, and Quality and Outcomes.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
