Ivy Lee Jia Jia, Raffaella Buzzetti, Richard David Leslie, Paolo Pozzilli
{"title":"LADA 30 周年:一种不断发展的糖尿病,始终存在悬而未决的问题","authors":"Ivy Lee Jia Jia, Raffaella Buzzetti, Richard David Leslie, Paolo Pozzilli","doi":"10.1002/dmrr.3800","DOIUrl":null,"url":null,"abstract":"<p>The 30th anniversary of Latent Autoimmune Diabetes in Adults (LADA) is a remarkable milestone in diabetes mellitus research. Described for the first time in 1993, LADA disputes the traditional binary classification of diabetes, with autoimmune features (autoimmune-mediated <i>β</i>-cell destruction) like that of type 1 diabetes (T1D) yet with an adult-onset pattern not requiring insulin, at least initially and, therefore, resembling type 2 diabetes (T2D).<span><sup>1, 2</sup></span> Thus, commenced an extensive journey of scientific exploration. Although our understanding of LADA has grown substantially over this period, many questions surrounding LADA remain unresolved. Today, LADA patients constitute a significant fraction, that is, up to 12% of T2D patients, highlighting the pressing need to address these questions.<span><sup>3, 4</sup></span> This commentary discusses such questions, the ongoing efforts by scientists/physicians and future directions in search for answers.</p><p>Diagnosing LADA is challenging due to overlaps with other forms of diabetes, also making it hard to define categorical features. In fact, LADA is often initially misdiagnosed as T2D because of the resemblance in their clinical presentation.<span><sup>5</sup></span> Furthermore, heterogeneity within LADA adds to this diagnostic challenge.<span><sup>2, 6</sup></span> Given that LADA people must be identified early to ensure better outcomes in terms of HbA1c, co-morbidity and hypoglycaemia risk, the best strategy for such identification must be resolved.</p><p>Regarding the diagnostic criteria of LADA, the Immunology of Diabetes Society proposed it includes diabetes cases age ≥30 years, positive for at least one diabetes-associated autoantibody, and without insulin requirement for at least the first six months after diagnosis.<span><sup>5</sup></span> There are some weaknesses with this proposal. First, all criteria are non-categorical, and all the cut-off values are arbitrary, as pointed out by Groop et al.<span><sup>2, 6, 7</sup></span> Second, there are many factors relating to diagnostic autoantibodies (e.g., how positivity is defined and which autoantibody, despite the most common being an autoantibody against glutamic acid decarboxylase [GADA]).<span><sup>3, 7</sup></span> This issue is demonstrated by the significant variability in the percentage of LADA diagnosis among different groups of T2D-diagnosed adults, depending on the autoantibody type used for screening and method of ascertainment.<span><sup>3</sup></span> Third, the choice of whether and when to start insulin treatment is highly physician-dependent, as highlighted by Rajkumar et al.<span><sup>5, 8</sup></span> For these reasons, more precise standardised diagnostic criteria for LADA may be needed.</p><p>As for autoantibody testing, there are no current general recommendations for adult-onset diabetes. At present, autoantibody testing is only done if there is a strong suspicion of LADA in patients with normal or low BMI; by implication patients with high BMI are not checked as they are assumed not to have LADA, which we know is incorrect.<span><sup>9</sup></span> Pertinent to autoantibody testing, an international expert panel in their recent consensus statement on the management of LADA recommended GADA testing for all newly diagnosed T2D patients.<span><sup>3</sup></span> Theoretically, this would improve identification of LADA patients, but there are practical issues, for example, cost implications. The panel suggested that if there are cost limitations, patients should be selected for GADA testing based on a list of different clinical factors that increase the suspicion of LADA and not only based on BMI as with the current practice. As for GADA-negative individuals who are suspected of having LADA, the panel recommended testing them for other islet autoantibodies.<span><sup>3</sup></span> We believe this will be a viable answer to the above-mentioned question.</p><p>A further issue regarding LADA diagnosis concerns the identification of LADA at an earlier stage, even before it develops into clinical diabetes and, how can this be done. More studies to address this issue are required.</p><p>As in its definition, LADA patients still possess functioning <i>β</i>-cells when diagnosed, making effective and timely interventions crucial to preserve the residual insulin secretory capacity and improve metabolic control. However, given that there are no specific guidelines for LADA management, so appropriate management still needs answering.<span><sup>3</sup></span></p><p>To answer the question above, it is crucial to first know the roles of different interventions, including hypoglycaemic agents. Based on the limited studies available, the current understanding of the roles of hypoglycaemic agents in LADA is summarised in Table 1.<span><sup>3, 8, 10-13</sup></span> Like many hypoglycaemic agents, the roles of lifestyle modifications and immune interventions in LADA are unclear.<span><sup>3</sup></span> This clearly shows the need for a better understanding of these interventions. Of note, one question to explore is whether insulin therapy should be commenced early when there is still residual <i>β</i>-cell function.<span><sup>3</sup></span> Hence, more large-scale randomised clinical trials with long-term follow-up are required. This approach is in line with the conclusion of a Cochrane Review and was supported by the recent consensus statement on the management of LADA.<span><sup>3, 8</sup></span></p><p>Besides, due to heterogeneity within LADA, the management of LADA should be tailored to each patient to ensure optimal outcomes. The panel recommended modifying the American Diabetes Association/European Association for the Study of Diabetes (EASD) algorithm for T2D to be used for the management of LADA. They suggested separating patients into three categories of C-peptide levels, which reflect the <i>β</i>-cell function status of the patient, to determine therapeutic decisions, as outlined in Table 2.<span><sup>3, 14</sup></span> We think this is a rational way forward, as measuring C-peptide levels is widely accessible and inexpensive.<span><sup>3</sup></span> However, further studies, especially clinical trials, are needed to study the outcomes (there are no such trials to date).</p><p>It was observed that LADA patients' progression and long-term outcomes vary considerably, as some patients maintained their <i>β</i>-cell function for long periods, while in other patients it deteriorated quickly.<span><sup>3</sup></span></p><p>Factors relevant to this rapid deterioration include both the level of GADA titre, the initial C-peptide, and the quality of glycaemic control. First, UKPDS and other studies discovered an association between high GADA levels and a higher risk of progression towards insulin requirement.<span><sup>15, 16</sup></span> Second, a post hoc analysis of UKPDS revealed that the risk of LADA patients developing microvascular complications compared to T2D patients is lower at disease onset but can become higher as a result of poor glycaemic control. This implies that optimal control of glycaemia may prevent the risk of developing complications later.<span><sup>17</sup></span></p><p>It will be important to identify factors involved in the more rapid metabolic deterioration, which can be targeted and by what means, to improve long-term outcomes, including insulin dependency and risks of complications.</p><p>Remaining unanswered questions include the best name for LADA (recently described as slowly-evolving autoimmune diabetes (SAID)), the cause of LADA and the environmental triggers that start the autoimmune attack on pancreatic <i>β</i>-cells.<span><sup>5</sup></span></p><p>Whilst there is evidence of genetic involvement in LADA, including those shared with T1D, such as higher risk in carriers of certain HLA haplotypes and those shared with T2D, further confirmation is needed.<span><sup>3, 18</sup></span> The same also applies to the potential genetic differences between LADA and T1D and whether they are due to actual differences or to the fact that LADA represents a late onset T1D, at least from a genetic standpoint.<span><sup>19</sup></span> Furthermore, how these genetic factors influence LADA susceptibility and progression to disease remains unclear.</p><p>Some studies have revealed immunological alterations in LADA, which are essential to improve understanding of LADA's autoimmunity process and potentially inform immunomodulation strategies.<span><sup>5</sup></span> However, they are still not fully elucidated. Additionally, drawing parallels with the partial remission stage of T1D may provide insights into the balance between autoimmunity and immunometabolism regulation, which may contribute to the broader understanding of autoimmune diabetes and allow shared therapeutic strategies.</p><p>There are also knowledge gaps in LADA's epidemiology that need addressing. For example, if an increase in incidence is occurring, what are the differences between regions with low and high incidence rates of T1D, and furthermore, if there are gender differences. This may help identify risk factors.</p><p>Finally, elucidation of these issues as noted above could lead to prevent LADA, much as we would like to do for T1D in children.</p><p>In conclusion, the 30th anniversary of LADA illustrates our evolving understanding of diabetes. As we celebrate this milestone, we should look back at the past and recognise the knowledge gaps in our understanding of LADA, some of which have been discussed in this commentary and are summarised in Table 3. However, it is essential to note that this commentary only discussed a tiny fraction of all the unresolved questions, as summarised in Figure 1. Looking to the future of LADA, we hope that the current momentum of scientific efforts will continue with more international collaborations in the next 3 decades, which, combined with advancements in technology, to answer most, if not all, of the unresolved questions to benefit our patients.</p><p>Ivy Lee Jia, Raffaella Buzzetti, Richard David Leslie and Paolo Pozzilli have equally contributed to the conceptualization, writing—original draft, review and editing, approval of the final version submitted for publication.</p><p>No potential conflicts of interest relevant to this paper were reported for Ivy Lee Jia, Raffaella Buzzetti, Richard David Leslie and Paolo Pozzilli.</p><p>This is a review article on a topic of general interest that does not require any approval by Ethical Committee.</p><p>Ivy Lee Jia Jia, Raffaella Buzzetti, Richard David Leslie and Paolo Pozzilli have nothing to disclose.</p>","PeriodicalId":11335,"journal":{"name":"Diabetes/Metabolism Research and Reviews","volume":"40 4","pages":""},"PeriodicalIF":6.0000,"publicationDate":"2024-04-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/dmrr.3800","citationCount":"0","resultStr":"{\"title\":\"LADA 30th anniversary: A growing form of diabetes with persistent unresolved questions\",\"authors\":\"Ivy Lee Jia Jia, Raffaella Buzzetti, Richard David Leslie, Paolo Pozzilli\",\"doi\":\"10.1002/dmrr.3800\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>The 30th anniversary of Latent Autoimmune Diabetes in Adults (LADA) is a remarkable milestone in diabetes mellitus research. Described for the first time in 1993, LADA disputes the traditional binary classification of diabetes, with autoimmune features (autoimmune-mediated <i>β</i>-cell destruction) like that of type 1 diabetes (T1D) yet with an adult-onset pattern not requiring insulin, at least initially and, therefore, resembling type 2 diabetes (T2D).<span><sup>1, 2</sup></span> Thus, commenced an extensive journey of scientific exploration. Although our understanding of LADA has grown substantially over this period, many questions surrounding LADA remain unresolved. Today, LADA patients constitute a significant fraction, that is, up to 12% of T2D patients, highlighting the pressing need to address these questions.<span><sup>3, 4</sup></span> This commentary discusses such questions, the ongoing efforts by scientists/physicians and future directions in search for answers.</p><p>Diagnosing LADA is challenging due to overlaps with other forms of diabetes, also making it hard to define categorical features. In fact, LADA is often initially misdiagnosed as T2D because of the resemblance in their clinical presentation.<span><sup>5</sup></span> Furthermore, heterogeneity within LADA adds to this diagnostic challenge.<span><sup>2, 6</sup></span> Given that LADA people must be identified early to ensure better outcomes in terms of HbA1c, co-morbidity and hypoglycaemia risk, the best strategy for such identification must be resolved.</p><p>Regarding the diagnostic criteria of LADA, the Immunology of Diabetes Society proposed it includes diabetes cases age ≥30 years, positive for at least one diabetes-associated autoantibody, and without insulin requirement for at least the first six months after diagnosis.<span><sup>5</sup></span> There are some weaknesses with this proposal. First, all criteria are non-categorical, and all the cut-off values are arbitrary, as pointed out by Groop et al.<span><sup>2, 6, 7</sup></span> Second, there are many factors relating to diagnostic autoantibodies (e.g., how positivity is defined and which autoantibody, despite the most common being an autoantibody against glutamic acid decarboxylase [GADA]).<span><sup>3, 7</sup></span> This issue is demonstrated by the significant variability in the percentage of LADA diagnosis among different groups of T2D-diagnosed adults, depending on the autoantibody type used for screening and method of ascertainment.<span><sup>3</sup></span> Third, the choice of whether and when to start insulin treatment is highly physician-dependent, as highlighted by Rajkumar et al.<span><sup>5, 8</sup></span> For these reasons, more precise standardised diagnostic criteria for LADA may be needed.</p><p>As for autoantibody testing, there are no current general recommendations for adult-onset diabetes. At present, autoantibody testing is only done if there is a strong suspicion of LADA in patients with normal or low BMI; by implication patients with high BMI are not checked as they are assumed not to have LADA, which we know is incorrect.<span><sup>9</sup></span> Pertinent to autoantibody testing, an international expert panel in their recent consensus statement on the management of LADA recommended GADA testing for all newly diagnosed T2D patients.<span><sup>3</sup></span> Theoretically, this would improve identification of LADA patients, but there are practical issues, for example, cost implications. The panel suggested that if there are cost limitations, patients should be selected for GADA testing based on a list of different clinical factors that increase the suspicion of LADA and not only based on BMI as with the current practice. As for GADA-negative individuals who are suspected of having LADA, the panel recommended testing them for other islet autoantibodies.<span><sup>3</sup></span> We believe this will be a viable answer to the above-mentioned question.</p><p>A further issue regarding LADA diagnosis concerns the identification of LADA at an earlier stage, even before it develops into clinical diabetes and, how can this be done. More studies to address this issue are required.</p><p>As in its definition, LADA patients still possess functioning <i>β</i>-cells when diagnosed, making effective and timely interventions crucial to preserve the residual insulin secretory capacity and improve metabolic control. However, given that there are no specific guidelines for LADA management, so appropriate management still needs answering.<span><sup>3</sup></span></p><p>To answer the question above, it is crucial to first know the roles of different interventions, including hypoglycaemic agents. Based on the limited studies available, the current understanding of the roles of hypoglycaemic agents in LADA is summarised in Table 1.<span><sup>3, 8, 10-13</sup></span> Like many hypoglycaemic agents, the roles of lifestyle modifications and immune interventions in LADA are unclear.<span><sup>3</sup></span> This clearly shows the need for a better understanding of these interventions. Of note, one question to explore is whether insulin therapy should be commenced early when there is still residual <i>β</i>-cell function.<span><sup>3</sup></span> Hence, more large-scale randomised clinical trials with long-term follow-up are required. This approach is in line with the conclusion of a Cochrane Review and was supported by the recent consensus statement on the management of LADA.<span><sup>3, 8</sup></span></p><p>Besides, due to heterogeneity within LADA, the management of LADA should be tailored to each patient to ensure optimal outcomes. The panel recommended modifying the American Diabetes Association/European Association for the Study of Diabetes (EASD) algorithm for T2D to be used for the management of LADA. They suggested separating patients into three categories of C-peptide levels, which reflect the <i>β</i>-cell function status of the patient, to determine therapeutic decisions, as outlined in Table 2.<span><sup>3, 14</sup></span> We think this is a rational way forward, as measuring C-peptide levels is widely accessible and inexpensive.<span><sup>3</sup></span> However, further studies, especially clinical trials, are needed to study the outcomes (there are no such trials to date).</p><p>It was observed that LADA patients' progression and long-term outcomes vary considerably, as some patients maintained their <i>β</i>-cell function for long periods, while in other patients it deteriorated quickly.<span><sup>3</sup></span></p><p>Factors relevant to this rapid deterioration include both the level of GADA titre, the initial C-peptide, and the quality of glycaemic control. First, UKPDS and other studies discovered an association between high GADA levels and a higher risk of progression towards insulin requirement.<span><sup>15, 16</sup></span> Second, a post hoc analysis of UKPDS revealed that the risk of LADA patients developing microvascular complications compared to T2D patients is lower at disease onset but can become higher as a result of poor glycaemic control. This implies that optimal control of glycaemia may prevent the risk of developing complications later.<span><sup>17</sup></span></p><p>It will be important to identify factors involved in the more rapid metabolic deterioration, which can be targeted and by what means, to improve long-term outcomes, including insulin dependency and risks of complications.</p><p>Remaining unanswered questions include the best name for LADA (recently described as slowly-evolving autoimmune diabetes (SAID)), the cause of LADA and the environmental triggers that start the autoimmune attack on pancreatic <i>β</i>-cells.<span><sup>5</sup></span></p><p>Whilst there is evidence of genetic involvement in LADA, including those shared with T1D, such as higher risk in carriers of certain HLA haplotypes and those shared with T2D, further confirmation is needed.<span><sup>3, 18</sup></span> The same also applies to the potential genetic differences between LADA and T1D and whether they are due to actual differences or to the fact that LADA represents a late onset T1D, at least from a genetic standpoint.<span><sup>19</sup></span> Furthermore, how these genetic factors influence LADA susceptibility and progression to disease remains unclear.</p><p>Some studies have revealed immunological alterations in LADA, which are essential to improve understanding of LADA's autoimmunity process and potentially inform immunomodulation strategies.<span><sup>5</sup></span> However, they are still not fully elucidated. Additionally, drawing parallels with the partial remission stage of T1D may provide insights into the balance between autoimmunity and immunometabolism regulation, which may contribute to the broader understanding of autoimmune diabetes and allow shared therapeutic strategies.</p><p>There are also knowledge gaps in LADA's epidemiology that need addressing. For example, if an increase in incidence is occurring, what are the differences between regions with low and high incidence rates of T1D, and furthermore, if there are gender differences. This may help identify risk factors.</p><p>Finally, elucidation of these issues as noted above could lead to prevent LADA, much as we would like to do for T1D in children.</p><p>In conclusion, the 30th anniversary of LADA illustrates our evolving understanding of diabetes. As we celebrate this milestone, we should look back at the past and recognise the knowledge gaps in our understanding of LADA, some of which have been discussed in this commentary and are summarised in Table 3. However, it is essential to note that this commentary only discussed a tiny fraction of all the unresolved questions, as summarised in Figure 1. Looking to the future of LADA, we hope that the current momentum of scientific efforts will continue with more international collaborations in the next 3 decades, which, combined with advancements in technology, to answer most, if not all, of the unresolved questions to benefit our patients.</p><p>Ivy Lee Jia, Raffaella Buzzetti, Richard David Leslie and Paolo Pozzilli have equally contributed to the conceptualization, writing—original draft, review and editing, approval of the final version submitted for publication.</p><p>No potential conflicts of interest relevant to this paper were reported for Ivy Lee Jia, Raffaella Buzzetti, Richard David Leslie and Paolo Pozzilli.</p><p>This is a review article on a topic of general interest that does not require any approval by Ethical Committee.</p><p>Ivy Lee Jia Jia, Raffaella Buzzetti, Richard David Leslie and Paolo Pozzilli have nothing to disclose.</p>\",\"PeriodicalId\":11335,\"journal\":{\"name\":\"Diabetes/Metabolism Research and Reviews\",\"volume\":\"40 4\",\"pages\":\"\"},\"PeriodicalIF\":6.0000,\"publicationDate\":\"2024-04-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/dmrr.3800\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Diabetes/Metabolism Research and Reviews\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/dmrr.3800\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diabetes/Metabolism Research and Reviews","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/dmrr.3800","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
LADA 30th anniversary: A growing form of diabetes with persistent unresolved questions
The 30th anniversary of Latent Autoimmune Diabetes in Adults (LADA) is a remarkable milestone in diabetes mellitus research. Described for the first time in 1993, LADA disputes the traditional binary classification of diabetes, with autoimmune features (autoimmune-mediated β-cell destruction) like that of type 1 diabetes (T1D) yet with an adult-onset pattern not requiring insulin, at least initially and, therefore, resembling type 2 diabetes (T2D).1, 2 Thus, commenced an extensive journey of scientific exploration. Although our understanding of LADA has grown substantially over this period, many questions surrounding LADA remain unresolved. Today, LADA patients constitute a significant fraction, that is, up to 12% of T2D patients, highlighting the pressing need to address these questions.3, 4 This commentary discusses such questions, the ongoing efforts by scientists/physicians and future directions in search for answers.
Diagnosing LADA is challenging due to overlaps with other forms of diabetes, also making it hard to define categorical features. In fact, LADA is often initially misdiagnosed as T2D because of the resemblance in their clinical presentation.5 Furthermore, heterogeneity within LADA adds to this diagnostic challenge.2, 6 Given that LADA people must be identified early to ensure better outcomes in terms of HbA1c, co-morbidity and hypoglycaemia risk, the best strategy for such identification must be resolved.
Regarding the diagnostic criteria of LADA, the Immunology of Diabetes Society proposed it includes diabetes cases age ≥30 years, positive for at least one diabetes-associated autoantibody, and without insulin requirement for at least the first six months after diagnosis.5 There are some weaknesses with this proposal. First, all criteria are non-categorical, and all the cut-off values are arbitrary, as pointed out by Groop et al.2, 6, 7 Second, there are many factors relating to diagnostic autoantibodies (e.g., how positivity is defined and which autoantibody, despite the most common being an autoantibody against glutamic acid decarboxylase [GADA]).3, 7 This issue is demonstrated by the significant variability in the percentage of LADA diagnosis among different groups of T2D-diagnosed adults, depending on the autoantibody type used for screening and method of ascertainment.3 Third, the choice of whether and when to start insulin treatment is highly physician-dependent, as highlighted by Rajkumar et al.5, 8 For these reasons, more precise standardised diagnostic criteria for LADA may be needed.
As for autoantibody testing, there are no current general recommendations for adult-onset diabetes. At present, autoantibody testing is only done if there is a strong suspicion of LADA in patients with normal or low BMI; by implication patients with high BMI are not checked as they are assumed not to have LADA, which we know is incorrect.9 Pertinent to autoantibody testing, an international expert panel in their recent consensus statement on the management of LADA recommended GADA testing for all newly diagnosed T2D patients.3 Theoretically, this would improve identification of LADA patients, but there are practical issues, for example, cost implications. The panel suggested that if there are cost limitations, patients should be selected for GADA testing based on a list of different clinical factors that increase the suspicion of LADA and not only based on BMI as with the current practice. As for GADA-negative individuals who are suspected of having LADA, the panel recommended testing them for other islet autoantibodies.3 We believe this will be a viable answer to the above-mentioned question.
A further issue regarding LADA diagnosis concerns the identification of LADA at an earlier stage, even before it develops into clinical diabetes and, how can this be done. More studies to address this issue are required.
As in its definition, LADA patients still possess functioning β-cells when diagnosed, making effective and timely interventions crucial to preserve the residual insulin secretory capacity and improve metabolic control. However, given that there are no specific guidelines for LADA management, so appropriate management still needs answering.3
To answer the question above, it is crucial to first know the roles of different interventions, including hypoglycaemic agents. Based on the limited studies available, the current understanding of the roles of hypoglycaemic agents in LADA is summarised in Table 1.3, 8, 10-13 Like many hypoglycaemic agents, the roles of lifestyle modifications and immune interventions in LADA are unclear.3 This clearly shows the need for a better understanding of these interventions. Of note, one question to explore is whether insulin therapy should be commenced early when there is still residual β-cell function.3 Hence, more large-scale randomised clinical trials with long-term follow-up are required. This approach is in line with the conclusion of a Cochrane Review and was supported by the recent consensus statement on the management of LADA.3, 8
Besides, due to heterogeneity within LADA, the management of LADA should be tailored to each patient to ensure optimal outcomes. The panel recommended modifying the American Diabetes Association/European Association for the Study of Diabetes (EASD) algorithm for T2D to be used for the management of LADA. They suggested separating patients into three categories of C-peptide levels, which reflect the β-cell function status of the patient, to determine therapeutic decisions, as outlined in Table 2.3, 14 We think this is a rational way forward, as measuring C-peptide levels is widely accessible and inexpensive.3 However, further studies, especially clinical trials, are needed to study the outcomes (there are no such trials to date).
It was observed that LADA patients' progression and long-term outcomes vary considerably, as some patients maintained their β-cell function for long periods, while in other patients it deteriorated quickly.3
Factors relevant to this rapid deterioration include both the level of GADA titre, the initial C-peptide, and the quality of glycaemic control. First, UKPDS and other studies discovered an association between high GADA levels and a higher risk of progression towards insulin requirement.15, 16 Second, a post hoc analysis of UKPDS revealed that the risk of LADA patients developing microvascular complications compared to T2D patients is lower at disease onset but can become higher as a result of poor glycaemic control. This implies that optimal control of glycaemia may prevent the risk of developing complications later.17
It will be important to identify factors involved in the more rapid metabolic deterioration, which can be targeted and by what means, to improve long-term outcomes, including insulin dependency and risks of complications.
Remaining unanswered questions include the best name for LADA (recently described as slowly-evolving autoimmune diabetes (SAID)), the cause of LADA and the environmental triggers that start the autoimmune attack on pancreatic β-cells.5
Whilst there is evidence of genetic involvement in LADA, including those shared with T1D, such as higher risk in carriers of certain HLA haplotypes and those shared with T2D, further confirmation is needed.3, 18 The same also applies to the potential genetic differences between LADA and T1D and whether they are due to actual differences or to the fact that LADA represents a late onset T1D, at least from a genetic standpoint.19 Furthermore, how these genetic factors influence LADA susceptibility and progression to disease remains unclear.
Some studies have revealed immunological alterations in LADA, which are essential to improve understanding of LADA's autoimmunity process and potentially inform immunomodulation strategies.5 However, they are still not fully elucidated. Additionally, drawing parallels with the partial remission stage of T1D may provide insights into the balance between autoimmunity and immunometabolism regulation, which may contribute to the broader understanding of autoimmune diabetes and allow shared therapeutic strategies.
There are also knowledge gaps in LADA's epidemiology that need addressing. For example, if an increase in incidence is occurring, what are the differences between regions with low and high incidence rates of T1D, and furthermore, if there are gender differences. This may help identify risk factors.
Finally, elucidation of these issues as noted above could lead to prevent LADA, much as we would like to do for T1D in children.
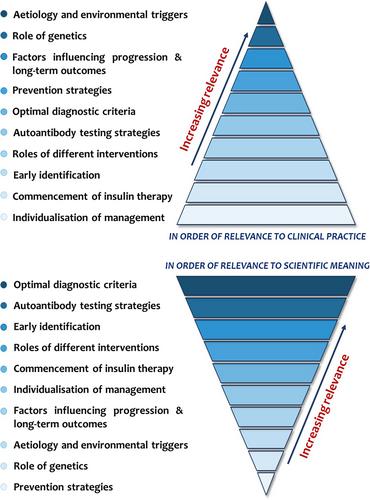
In conclusion, the 30th anniversary of LADA illustrates our evolving understanding of diabetes. As we celebrate this milestone, we should look back at the past and recognise the knowledge gaps in our understanding of LADA, some of which have been discussed in this commentary and are summarised in Table 3. However, it is essential to note that this commentary only discussed a tiny fraction of all the unresolved questions, as summarised in Figure 1. Looking to the future of LADA, we hope that the current momentum of scientific efforts will continue with more international collaborations in the next 3 decades, which, combined with advancements in technology, to answer most, if not all, of the unresolved questions to benefit our patients.
Ivy Lee Jia, Raffaella Buzzetti, Richard David Leslie and Paolo Pozzilli have equally contributed to the conceptualization, writing—original draft, review and editing, approval of the final version submitted for publication.
No potential conflicts of interest relevant to this paper were reported for Ivy Lee Jia, Raffaella Buzzetti, Richard David Leslie and Paolo Pozzilli.
This is a review article on a topic of general interest that does not require any approval by Ethical Committee.
Ivy Lee Jia Jia, Raffaella Buzzetti, Richard David Leslie and Paolo Pozzilli have nothing to disclose.
期刊介绍:
Diabetes/Metabolism Research and Reviews is a premier endocrinology and metabolism journal esteemed by clinicians and researchers alike. Encompassing a wide spectrum of topics including diabetes, endocrinology, metabolism, and obesity, the journal eagerly accepts submissions ranging from clinical studies to basic and translational research, as well as reviews exploring historical progress, controversial issues, and prominent opinions in the field. Join us in advancing knowledge and understanding in the realm of diabetes and metabolism.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
